

Localization of insulinomas to regions of the pancreas by intraarterial calcium stimulation: the NIH experience
- PMID: 19190102
- PMCID: PMC2682461
- DOI: 10.1210/jc.2008-1986
Localization of insulinomas to regions of the pancreas by intraarterial calcium stimulation: the NIH experience
Abstract
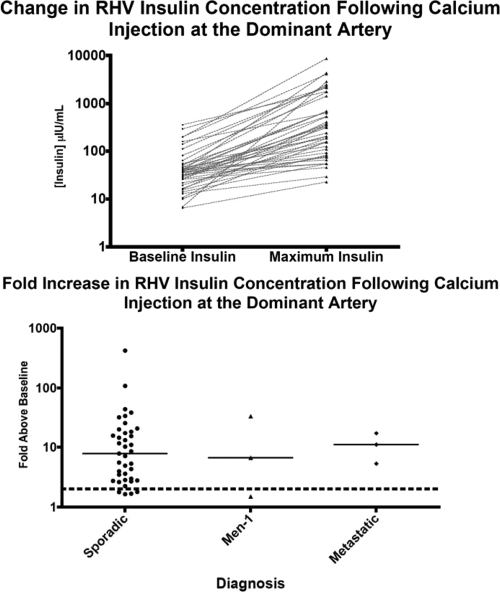
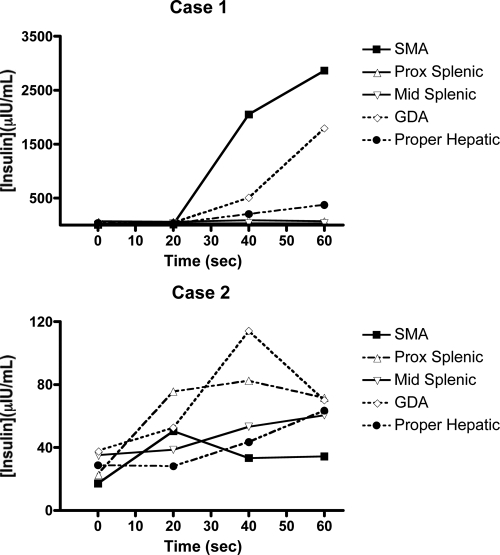
Context: Selective intraarterial calcium injection of the major pancreatic arteries with hepatic venous sampling [calcium arterial stimulation (CaStim)] has been used as a localizing tool for insulinomas at the National Institutes of Health (NIH) since 1989. The accuracy of this technique for localizing insulinomas was reported for all cases until 1996.
Objectives: The aim of the study was to assess the accuracy and track record of the CaStim over time and in the context of evolving technology and to review issues related to result interpretation and procedure complications. CaStim was the only invasive preoperative localization modality used at our center. Endoscopic ultrasound (US) was not studied.
Design and setting: We conducted a retrospective case review at a referral center.
Patients: Twenty-nine women and 16 men (mean age, 47 yr; range, 13-78) were diagnosed with an insulinoma from 1996-2008.
Intervention: A supervised fast was conducted to confirm the diagnosis of insulinoma. US, computed tomography (CT), magnetic resonance imaging (MRI), and CaStim were used as preoperative localization studies. Localization predicted by each preoperative test was compared to surgical localization for accuracy.
Main outcome: We measured the accuracy of US, CT, MRI, and CaStim for localization of insulinomas preoperatively.
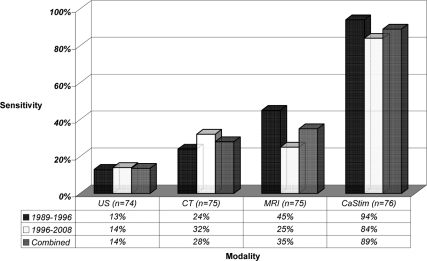
Results: All 45 patients had surgically proven insulinomas. Thirty-eight of 45 (84%) localized to the correct anatomical region by CaStim. In five of 45 (11%) patients, the CaStim was falsely negative. Two of 45 (4%) had false-positive localizations.
Conclusion: The CaStim has remained vastly superior to abdominal US, CT, or MRI over time as a preoperative localizing tool for insulinomas. The utility of the CaStim for this purpose and in this setting is thus validated.
Figures
References
-
- Service FJ, McMahon MM, O'Brien PC, Ballard DJ 1991 Functioning insulinoma—incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc 66:711–719 - PubMed
-
- Oberg K, Eriksson B 2005 Endocrine tumours of the pancreas. Best Pract Res Clin Gastroenterol 19:753–781 - PubMed
-
- Service FJ, Dale AJ, Elveback LR, Jiang NS 1976 Insulinoma: clinical and diagnostic features of 60 consecutive cases. Mayo Clin Proc 51:417–429 - PubMed
-
- Hirshberg B, Livi A, Bartlett DL, Libutti SK, Alexander HR, Doppman JL, Skarulis MC, Gorden P 2000 Forty-eight-hour fast: the diagnostic test for insulinoma. J Clin Endocrinol Metab 85:3222–3226 - PubMed
-
- Grama D, Eriksson B, Martensson H, Cedermark B, Ahren B, Kristoffersson A, Rastad J, Oberg K, Akerstrom G 1992 Clinical characteristics, treatment and survival in patients with pancreatic tumors causing hormonal syndromes. World J Surg 16:632–639 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
