

Incomplete peripheral CD4+ cell count restoration in HIV-infected patients receiving long-term antiretroviral treatment
- PMID: 19193107
- PMCID: PMC2720023
- DOI: 10.1086/597093
Incomplete peripheral CD4+ cell count restoration in HIV-infected patients receiving long-term antiretroviral treatment
Abstract
Background: Although antiretroviral therapy has the ability to fully restore a normal CD4(+) cell count (>500 cells/mm(3)) in most patients, it is not yet clear whether all patients can achieve normalization of their CD4(+) cell count, in part because no study has followed up patients for >7 years.
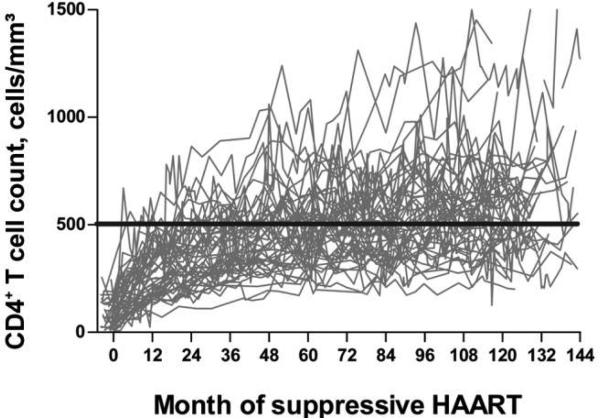
Methods: Three hundred sixty-six patients from 5 clinical cohorts who maintained a plasma human immunodeficiency virus (HIV) RNA level 1000 copies/mL for at least 4 years after initiation of antiretroviral therapy were included. Changes in CD4(+) cell count were evaluated using mixed-effects modeling, spline-smoothing regression, and Kaplan-Meier techniques.
Results: The majority (83%) of the patients were men. The median CD4(+) cell count at the time of therapy initiation was 201 cells/mm(3) (interquartile range, 72-344 cells/mm(3)), and the median age was 47 years. The median follow-up period was 7.5 years (interquartile range, 5.5-9.7 years). CD4(+) cell counts continued to increase throughout the follow-up period, albeit slowly after year 4. Although almost all patients (95%) who started therapy with a CD4(+) cell count 300 cells/mm(3) were able to attain a CD4(+) cell count 500 cells/mm(3), 44% of patients who started therapy with a CD4(+) cell count <100 cells/mm(3) and 25% of patients who started therapy with a CD4(+) cell count of 100-200 cells/mm(3) were unable to achieve a CD4(+) cell count >500 cells/mm(3) over a mean duration of follow-up of 7.5 years; many did not reach this threshold by year 10. Twenty-four percent of individuals with a CD4(+) cell count <500 cells/mm(3) at year 4 had evidence of a CD4(+) cell count plateau after year 4. The frequency of detectable viremia ("blips") after year 4 was not associated with the magnitude of the CD4(+) cell count change.
Conclusions: A substantial proportion of patients who delay therapy until their CD4(+) cell count decreases to <200 cells/mm(3) do not achieve a normal CD4(+) cell count, even after a decade of otherwise effective antiretroviral therapy. Although the majority of patients have evidence of slow increases in their CD4(+) cell count over time, many do not. These individuals may have an elevated risk of non-AIDS-related morbidity and mortality.
Figures



Comment in
-
The paradox of incomplete CD4+ cell count restoration despite successful antiretroviral treatment and the need to start highly active antiretroviral therapy early.Clin Infect Dis. 2009 Mar 15;48(6):795-7. doi: 10.1086/597094. Clin Infect Dis. 2009. PMID: 19196173 No abstract available.
References
-
- Battegay M, Nuesch R, Hirschel B, Kaufmann GR. Immunological recovery and antiretroviral therapy in HIV-1 infection. Lancet Infect Dis. 2006;6:280–7. - PubMed
-
- Pakker NG, Notermans DW, de Boer RJ, et al. Biphasic kinetics of peripheral blood T cells after triple combination therapy in HIV-1 infection: a composite of redistribution and proliferation. Nat Med. 1998;4:208–14. - PubMed
-
- Garcia F, de Lazzari E, Plana M, et al. Long-term CD4+ T-cell response to highly active antiretroviral therapy according to baseline CD4+ T-cell count. J Acquir Immune Defic Syndr. 2004;36:702–13. - PubMed
-
- Moore RD, Keruly JC. CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin Infect Dis. 2007;44:441–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AI027767/AI/NIAID NIH HHS/United States
- AI41531/AI/NIAID NIH HHS/United States
- AI067039/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- AI071713/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- AI27763/AI/NIAID NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- MH59037/MH/NIMH NIH HHS/United States
- P01 AI071713/AI/NIAID NIH HHS/United States
- T32 AI007140/AI/NIAID NIH HHS/United States
- K24 AI069994/AI/NIAID NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- P30 MH059037/MH/NIMH NIH HHS/United States
- U01 AI041531/AI/NIAID NIH HHS/United States
- AI-36219/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
