

HIV preexposure prophylaxis in the United States: impact on lifetime infection risk, clinical outcomes, and cost-effectiveness
- PMID: 19193111
- PMCID: PMC2876329
- DOI: 10.1086/597095
HIV preexposure prophylaxis in the United States: impact on lifetime infection risk, clinical outcomes, and cost-effectiveness
Abstract
Background: The combination of tenofovir and emtricitabine shows promise as HIV preexposure prophylaxis (PrEP). We sought to forecast clinical, epidemiologic, and economic outcomes of PrEP, taking into account uncertainties regarding efficacy, the risks of developing drug resistance and toxicity, behavioral disinhibition, and drug costs.
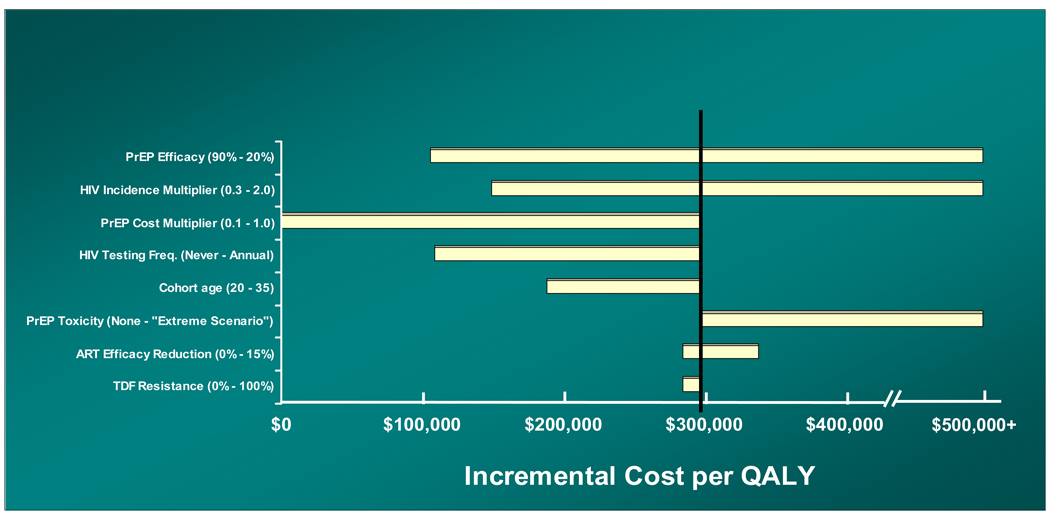
Methods: We adapted a computer simulation of HIV acquisition, detection, and care to model PrEP among men who have sex with men and are at high risk of HIV infection (i.e., 1.6% mean annual incidence of HIV infection) in the United States. Base-case assumptions included 50% PrEP efficacy and monthly tenofovir-emtricitabine costs of $753. We used sensitivity analyses to examine the stability of results and to identify critical input parameters.
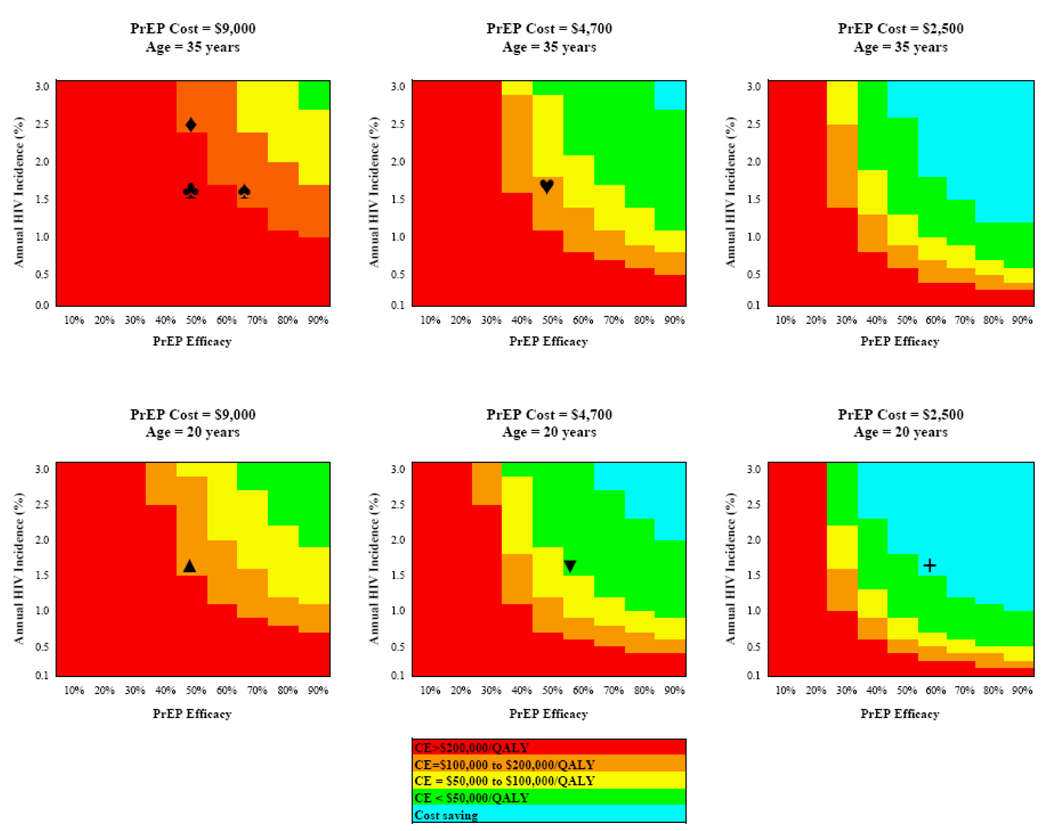
Results: In a cohort with a mean age of 34 years, PrEP reduced lifetime HIV infection risk from 44% to 25% and increased mean life expectancy from 39.9 to 40.7 years (21.7 to 22.2 discounted quality-adjusted life-years). Discounted mean lifetime treatment costs increased from $81,100 to $232,700 per person, indicating an incremental cost-effectiveness ratio of $298,000 per quality-adjusted life-year gained. Markedly larger reductions in lifetime infection risk (from 44% to 6%) were observed with the assumption of greater (90%) PrEP efficacy. More-favorable incremental cost-effectiveness ratios were obtained by targeting younger populations with a higher incidence of infection and by improvements in the efficacy and cost of PrEP.
Conclusions: PrEP could substantially reduce the incidence of HIV transmission in populations at high risk of HIV infection in the United States. Although it is unlikely to confer sufficient benefits to justify the current costs of tenofovir-emtricitabine, price reductions and/or increases in efficacy could make PrEP a cost-effective option in younger populations or populations at higher risk of infection. Given recent disappointments in HIV infection prevention and vaccine development, additional study of PrEP-based HIV prevention is warranted.
Conflict of interest statement
With the exception of Dr. Sax, none of the authors report any association that might pose a conflict of interest (e.g., pharmaceutical stock ownership, consultancy, advisory board membership, relevant patents, or research funding). Dr. Sax serves as a Consultant to Abbott, BMS, Gilead, GSK, Merck, and Tibotec. He receives honoraria for teaching from Abbott, BMS, Gilead, Merck, Tibotec. He receives grant support from Merck.
Figures
References
-
- Walensky RP, Paltiel AD, Losina E, et al. Three million years of life saved: The survival benefits of AIDS treatment in the United States. J Infect Dis. 2006 Jul 1;194(1):11–19. - PubMed
-
- Doncel G, van Damme L. Update on the CONRAD cellulose sulfate trial [Abstract 106LB]. 14th Conference on Retroviruses and Opportunistic Infections; Los Angeles, CA. 2007.
-
- World Health Organization. Cellulose sulfate microbicide trial stopped. 2007. Jan 31 [cited February 1 2008]. Available from: http://www.who.int/mediacentre/news/statements/2007/s01/en/index.html.
Publication types
MeSH terms
Substances
Grants and funding
- R37 AI042006/AI/NIAID NIH HHS/United States
- K25AI50436/AI/NIAID NIH HHS/United States
- R01 MH065869/MH/NIMH NIH HHS/United States
- P30 AI042851/AI/NIAID NIH HHS/United States
- R37AI42006/AI/NIAID NIH HHS/United States
- K25 AI050436/AI/NIAID NIH HHS/United States
- K01 DA017179/DA/NIDA NIH HHS/United States
- R01 DA015612/DA/NIDA NIH HHS/United States
- R01MH65869/MH/NIMH NIH HHS/United States
- K24AI062476/AI/NIAID NIH HHS/United States
- P30AI42851/AI/NIAID NIH HHS/United States
- K01DA17179/DA/NIDA NIH HHS/United States
- R01DA015612/DA/NIDA NIH HHS/United States
- K24 AI062476/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
