

Bailout stent deployment during coil embolization of intracranial aneurysms
- PMID: 19193745
- PMCID: PMC7051677
- DOI: 10.3174/ajnr.A1482
Bailout stent deployment during coil embolization of intracranial aneurysms
Abstract
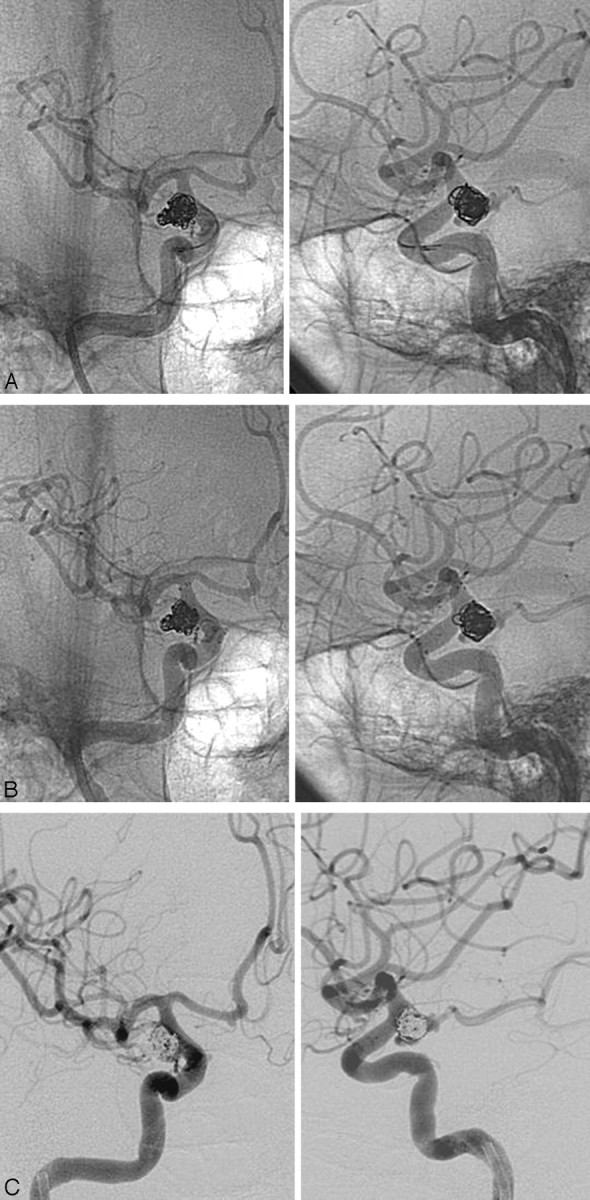
Background and purpose: Self-expandable stents are an effective tool for coil embolization of wide-neck intracranial aneurysms. The purpose of this study was to assess the feasibility and results of bailout stent positioning during rescue situations after deployment of > or =1 coil.
Materials and methods: Among 318 aneurysms treated by coil embolization in 267 patients, 16 patients who were treated by bailout stent deployment were retrospectively reviewed. Bailout procedures were performed to relieve potential parent artery compromise caused by the protruded coil loops or to prevent migration of the unstable coil basket. The size/location of the aneurysm, technical feasibility, successful stabilization rate, and procedure-related complications were evaluated.
Results: The locations of the aneurysms were the internal carotid artery (n = 12) and basilar artery (n = 4). The mean aneurysm size was 8.3 mm (range, 3.5-19.4 mm) with hemorrhagic presentation in 3 patients. Relief/prevention of parent artery compromise was achieved by molding the encroached loops back into the sac (n = 11), scaffolding the aneurysmal neck in cases with an unstable coil basket (n = 4), and sidetacking the migrated loop to the parent vessel wall (n = 1). The procedure was technically successful in 87.5% (n = 14). Satisfactory molding or stabilization of the coil was seen in 75% (n = 12). Unsatisfactory molding of the protruded small coil loop was noted in 2 cases of small aneurysms. Acute in-stent thrombosis was successfully managed by thrombolysis (n = 1).
Conclusions: Bailout self-expandable stent deployment may be a feasible and effective method for relief/prevention of parent artery compromise or coil migration caused by prolapsed or unstable coil loops during embolization of aneurysms.
Figures

References
-
- Fessler RD, Ringer AJ, Qureshi AI, et al. Intracranial stent placement to trap an extruded coil during endovascular aneurysm treatment: technical note Neurosurgery 2000;46:248–51, discussion 251–53 - PubMed
-
- Vinuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475–82 - PubMed
-
- Benitez RP, Silva MT, Klem J, et al. Endovascular occlusion of wide-necked aneurysms with a new intracranial microstent (Neuroform) and detachable coils. Neurosurgery 2004;54:1359–67, discussion 1368 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical