

Two-year virologic outcomes of an alternative AIDS care model: evaluation of a peer health worker and nurse-staffed community-based program in Uganda
- PMID: 19194316
- PMCID: PMC2662625
- DOI: 10.1097/QAI.0b013e3181988375
Two-year virologic outcomes of an alternative AIDS care model: evaluation of a peer health worker and nurse-staffed community-based program in Uganda
Abstract
Background: There is growing concern about the human resources needed to care for increasing numbers of patients receiving antiretroviral therapy in resource-limited settings. We evaluated an alternative model, community-based, comprehensive antiretroviral program staffed primarily by peer health workers and nurses.
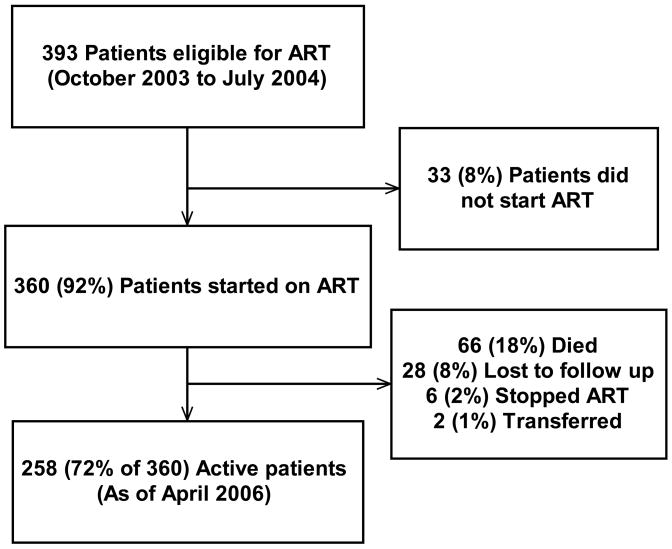
Methods: We conducted a retrospective cohort study of patients receiving antiretroviral therapy during the first 10 months of program enrollment beginning in late 2003. Virologic, immunologic, clinical, and adherence data were collected.
Results: Of 360 patients started on treatment, 258 (72%) were active and on therapy approximately 2 years later. Viral load testing demonstrated that 86% of active patients (211/246 tested) had a viral load <400 copies per milliliter. The median CD4 increase for active patients was 197 cells per cubic millimeter (interquartile range, 108-346). Patients with either a history of antiretroviral use or lack of CD4 response were more likely to experience virologic failure. Survival was 84% at 1 year and 82% at 2 years. World Health Organization stage 4 was predictive of both not sustaining therapy and increased mortality.
Conclusions: A community-based antiretroviral treatment program in a resource-limited setting can provide excellent AIDS care over at least a 2-year period. A comprehensive program based upon peer health workers and nurses provides an effective alternative model for AIDS care.
Figures


References
-
- Van Damme W, Kober K, Laga M. The real challenges for scaling up ART in sub-Saharan Africa. Aids. 2006 Mar 21;20(5):653–656. - PubMed
-
- Colebunders R, Ronald A, Katabira E, Sande M. Rolling out antiretrovirals in Africa: there are still challenges ahead. Clin Infect Dis. 2005 Aug 1;41(3):386–389. - PubMed
-
- Staszewski S, Miller V, Sabin C, et al. Virological response to protease inhibitor therapy in an HIV clinic cohort. Aids. 1999 Feb 25;13(3):367–373. - PubMed
-
- Lucas GM, Chaisson RE, Moore RD. Highly active antiretroviral therapy in a large urban clinic: risk factors for virologic failure and adverse drug reactions. Ann Intern Med. 1999 Jul 20;131(2):81–87. - PubMed
-
- Deeks SG, Hecht FM, Swanson M, et al. HIV RNA and CD4 cell count response to protease inhibitor therapy in an urban AIDS clinic: response to both initial and salvage therapy. Aids. 1999 Apr 16;13(6):F35–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
