

Primary localized malignant biphasic mesothelioma of the liver in a patient with asbestosis
- PMID: 19195066
- PMCID: PMC2653355
- DOI: 10.3748/wjg.15.615
Primary localized malignant biphasic mesothelioma of the liver in a patient with asbestosis
Abstract
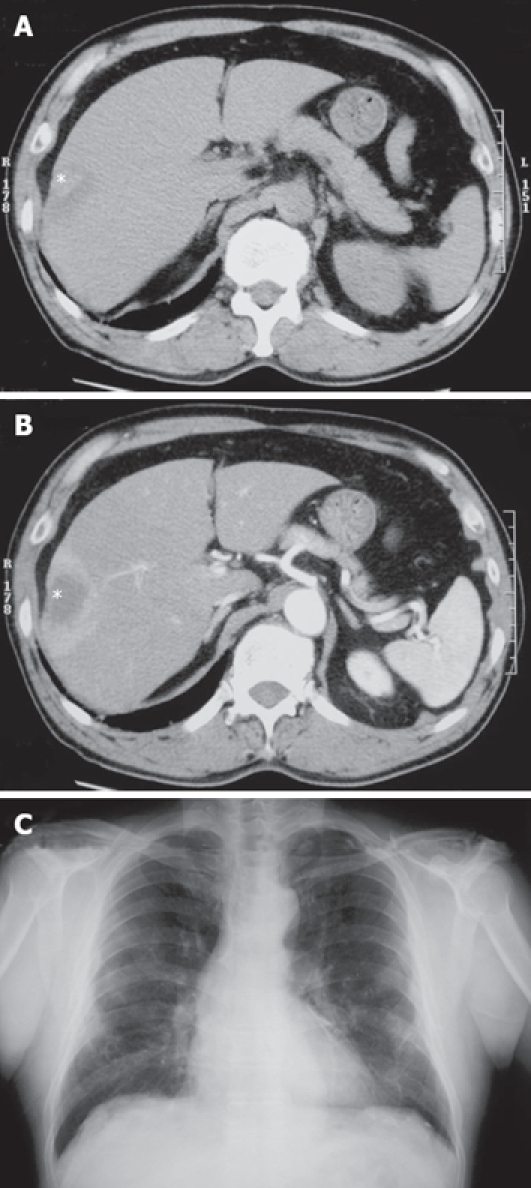
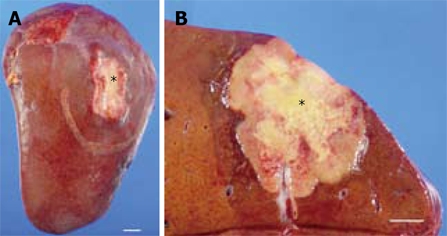
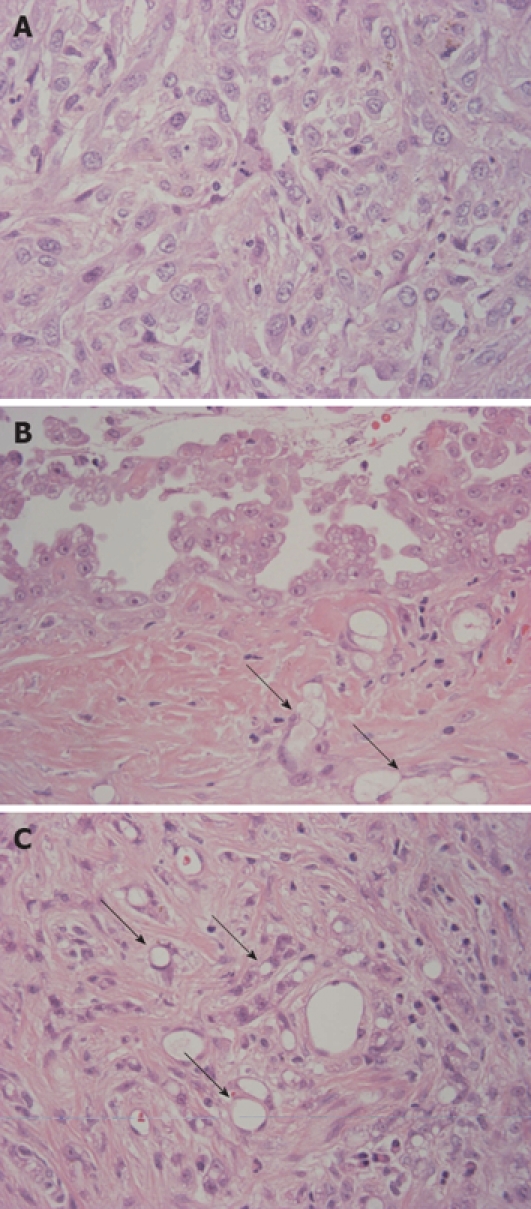
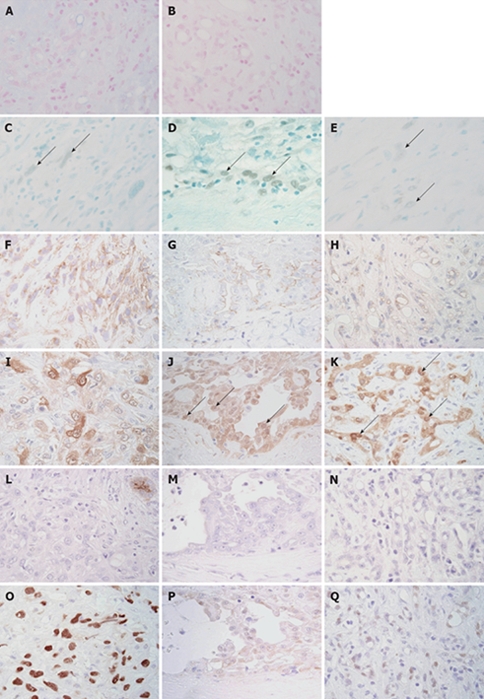
We report a case of primary localized malignant biphasic mesothelioma of the liver in a 66-year-old man associated with asbestosis. The tumor was detected as a hepatic nodule, 4 cm in diameter, in the right lobe (S8 segment) on CT scan. Histopathological examination demonstrated an intrahepatic tumor with central necrosis consisting of a papillary epithelioid pattern on the surface of the liver, microcystic (microglandular or adenomatoid) pattern mainly in the subcapsular area and sarcomatoid pattern intermingled with microcystic pattern in the major part of the hepatic nodular tumor. Tumor cells, especially of epithelioid type, showed distinct immunoreactivity for mesothelial markers (WT-1, calretinin, D2-40, CK5/6, mesothelin, thrombomodulin) and no immunoreactivity for epithelial (adenocarcinoma) markers (CEA, CD15, BerEP4, BG8, MOC31). P53 immunoreactivity was detected focally in papillary epithelioid tumor cells and extensively in microcystic and sarcomatoid components, suggesting that the papillary epithelioid mesothelioma arose on the surface of the liver, and tumor cells showing microcystic and sarcomatoid patterns invaded and grew into the liver. To date, this is the first case of primary localized malignant biphasic mesothelioma of the liver, since all three primary hepatic mesotheliomas reported so far were epithelioid type.
Figures
References
-
- Maitra A, Kumar V. The lung and upper respiratory tract. In: V Kumar, R Cotran, S Robbins., editors. Robbins Basic Pathology. 7th ed. Saunders: Philadelphia; 2002. pp. 453–509.
-
- Flemming P, Becker T, Klempnauer J, Högemann D, Kreft A, Kreipe HH. Benign cystic mesothelioma of the liver. Am J Surg Pathol. 2002;26:1523–1527. - PubMed
-
- Churg A, Roggli V, Galateau-Salle F, Cagle P, Gibbs A, Hasleton P, Henderson D, Vignaud J. Mesothelioma. In: W Travis, E Brambilla, H Muller-Hermelink, C Harris., editors. Pathology & Genetics Tumours of the Lung, Pleura, Thymus and Heart. IARC: Lyon; 2004. pp. 125–136.
-
- Marubayashi S, Ohdan H, Asahara T, Ikeda M, Hinoi T, Fukuma K, Maeda T, Oshiro Y, Shimamoto F, Dohi K. Malignant mesothelioma originating in the hepatic falciform ligament: report of a case. Surg Today. 1998;28:929–931. - PubMed
-
- Bierhoff E, Pfeifer U. Malignant mesothelioma arising from a benign mediastinal mesothelial cyst. Gen Diagn Pathol. 1996;142:59–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
