

Review
doi: 10.1016/j.rcl.2008.11.001.
The "post-64" era of coronary CT angiography: understanding new technology from physical principles
Affiliations
- PMID: 19195535
- PMCID: PMC2893874
- DOI: 10.1016/j.rcl.2008.11.001
Item in Clipboard
Review
The "post-64" era of coronary CT angiography: understanding new technology from physical principles
Radiol Clin North Am.
2009 Jan.
Abstract
Multidetector CT now provides noninvasive coronary imaging, and patients with a low or intermediate probability of coronary artery disease can be imaged with radiation levels comparable to catheterization. Cardiac imaging drives rapid progress in CT hardware. To best apply evolving technology, imagers and referring clinicians need a solid understanding of spatial resolution, temporal resolution, volume coverage, and radiation dose. This article defines and discusses interactions between these parameters for state-of-the-art CT.
Figures
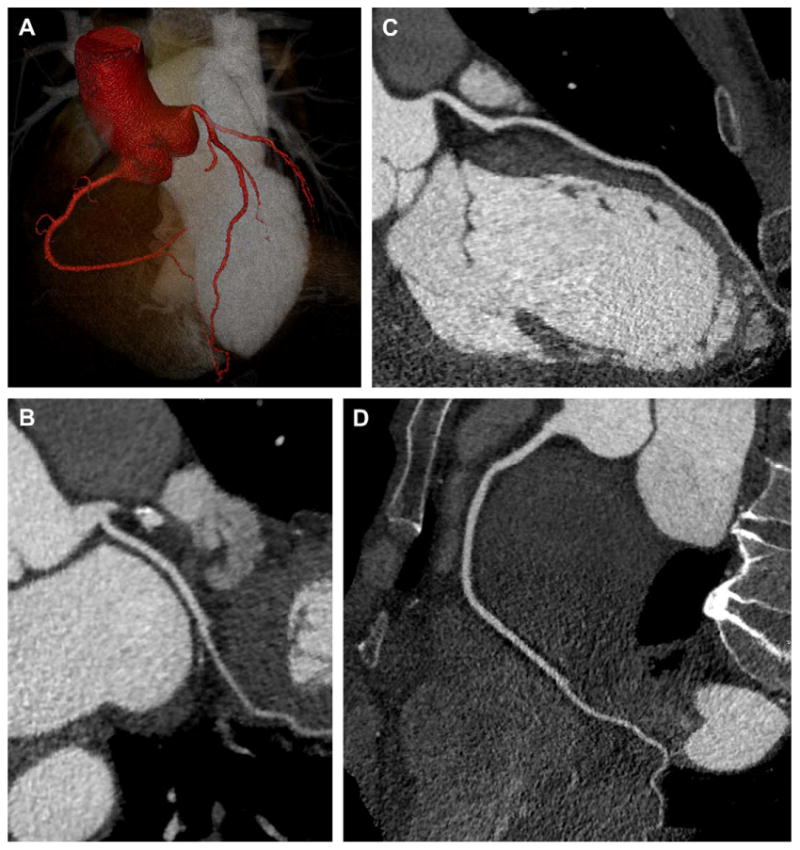
48-year-old woman with atypical chest pain and nonspecific ECG findings. Single heartbeat coronary imaging was performed using 320-slice CT (Toshiba AquilionOne, Tochigi-ken, Japan) with 100 kV, 400 mAs, 350 millisecond gantry rotation, and 80 mL of iopamidol 370 mg I/mL (Isovue-370, Bracco Diagnostics, Princeton, NJ). The use of prospective ECG gating (phase window width = 10%) and low kV (patient weight <170 pounds) enabled a 2.6 mSv acquisition. (A) 3D volume rendering (Vitrea fx, Vital Images, Minnetonka, MN) of the aortic root, major coronary arteries, and left ventricular cavity. (B, C, D) Curved multiplanar reformatted images of the normal coronary arteries.
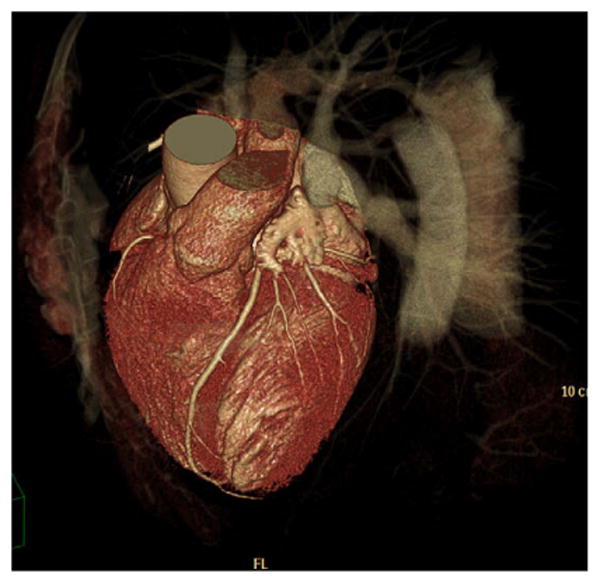
3D volume rendered image of a 62-year-old man with chest pain. CT was requested and excluded CAD. The patient was imaged with 256-slice CT, 128 detector rows and an alternating focal spot (Philips Brilliance iCT, Best, The Netherlands). With a scan time of 4 sec, 13 cm of craniocaudal coverage was achieved. (Courtesy of Nathan Peled, Carmel Medical Center, Haifa, Israel.)
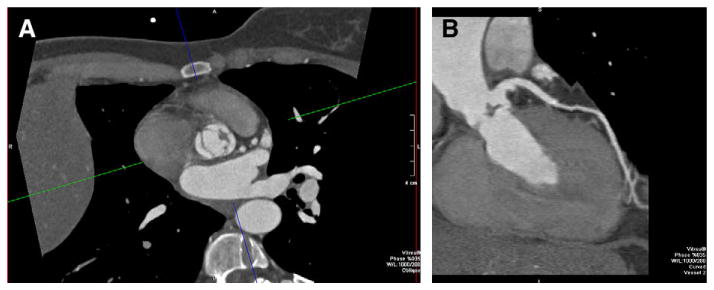
55-year-old man with abnormal aortic valve motion by echocardiography. CT was requested to exclude CAD. The patient's heart rate (>100 beats per minute at the time of acquisition) could not be safely lowered because of hypotension. (A) Retrospectively ECG gated dual-source cardiac CT (Siemens Definition, Erlangen, Germany) with 83 milliseconds temporal resolution depicted the vegetation of the aortic valve, as noted on the axial images. (B) Curved multiplanar reformatted image of the LAD also shows the vegetation in addition to demonstrating a normal LAD.
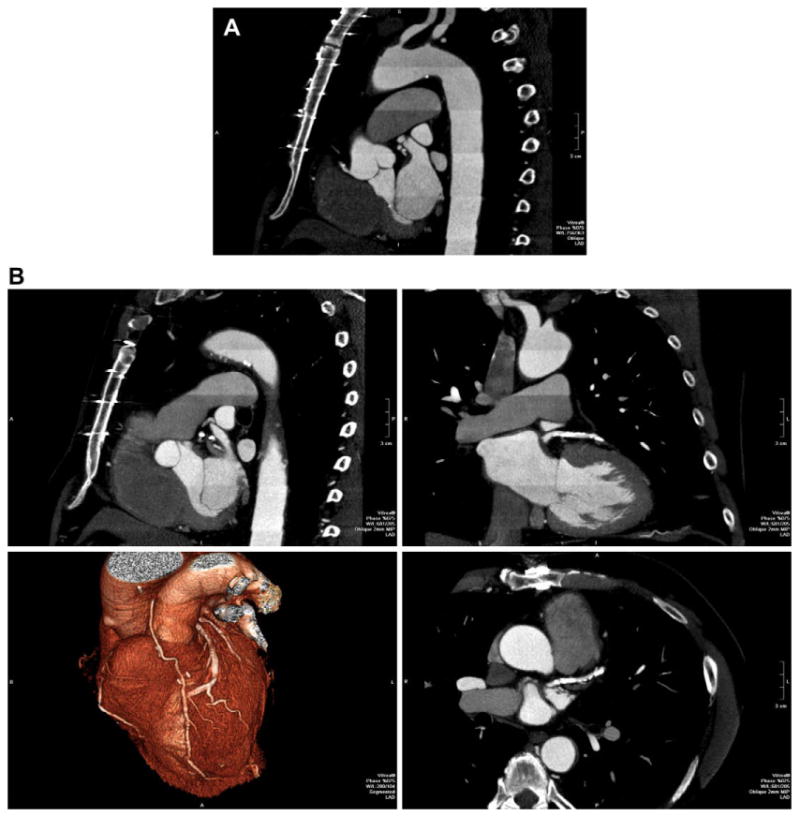
72-year-old man status post coronary artery bypass grafting. Because of the large craniocaudal field of view, imaging was performed over 13 heartbeats, 7 beats of data acquisition plus 6 move the patient within the gantry. This “step and shoot” technique significantly decreases the radiation exposure when compared to retrospective ECG gating. (A) Left anterior oblique reformation over the entire z-axis FOV shows high image quality. Enhancement pattern in the aorta demonstrates the individual “steps” as described. (B) Multiplanar reformatted images as well as 3D volume rendering (lower left) focused on the heavily calcified left anterior descending.
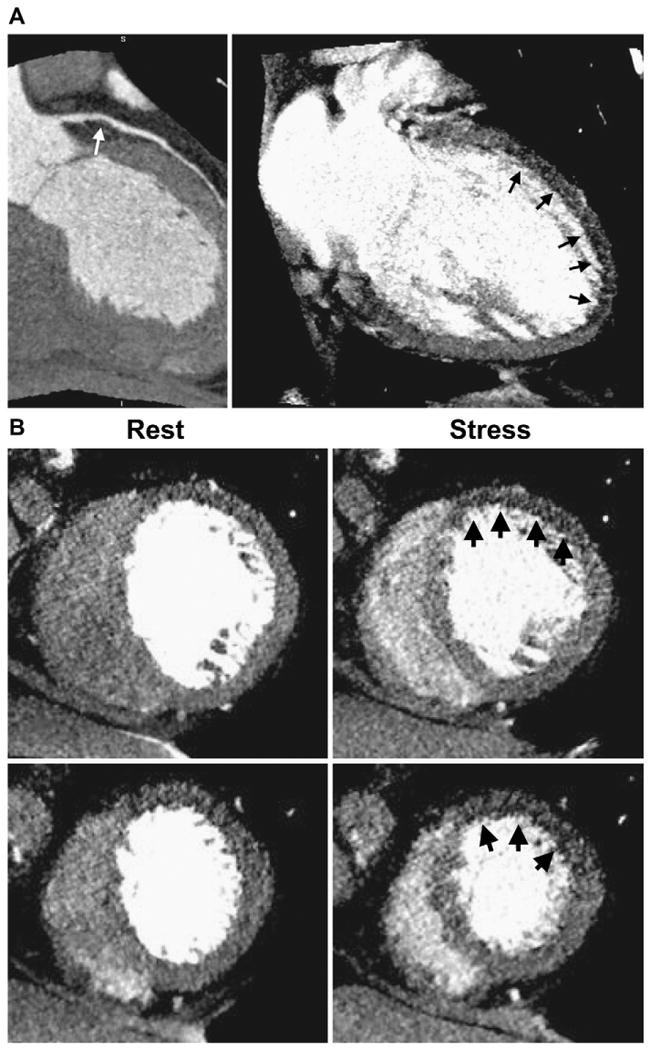
57-year-old woman with history hypertension and hyperlipidemia complaining of atypical chest pain. The patient underwent 320-detector row CT (Toshiba AquilionOne, Tochigi-ken, Japan) coronary CTA plus perfusion imaging. (A) CTA (left) followed by adenosine stress CT perfusion imaging (right). CTA shows a noncalcified plaque (white arrow) causing a moderate stenosis in the proximal LAD. Stress perfusion imaging (right) shows a subendocardial perfusion deficit in the anterior and apical walls (black arrows). (B) Short axis views reformatted with 3-mm slice thickness. Rest images (left) demonstrate very mild hypoattenuation in the anterior wall. Stress CT perfusion images (right) show perfusion deficit in the anterior wall at the level of the mid and distal left ventricle. (Courtesy of Richard T. George and Joao AC. Lima, Johns Hopkins University, Division of Cardiology.)
References
-
- Budof MJ, Dowe D, Jollis J, et al. Diagnostic Performance of 64-Multidetector Row Coronary Computed Tomographic Angiography for Evaluation of Coronary Artery Stenosis in Individuals Without Known Coronary Artery Disease: Results From the Prospective Multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) Trial. J Am Coll Cardiol. 2008;52:1724–32. - PubMed
-
- Miller JM, Rochitte CE, Dewey M, et al. Diagnostic Performance of Coronary Angiography by 64-Row CT. N Engl J Med. 2008;359:2324–36. - PubMed
-
- Achenbach S. Cardiac CT: state of the art for the detection of coronary arterial stenosis. J Cardiovascular Computed Tomography. 2007;1:3–20. - PubMed
-
- Hoffmann U, Pena AJ, Cury RC, et al. Cardiac CT in emergency department patients with acute chest pain. Radiographics. 2006;26:963–78. discussion: 979–80. - PubMed
-
- Flohr TG, McCollough CH, Bruder H, et al. First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol. 2006;16:256–68. - PubMed
