

Central sympatholytics prolong survival in experimental sepsis
- PMID: 19196475
- PMCID: PMC2688128
- DOI: 10.1186/cc7709
Central sympatholytics prolong survival in experimental sepsis
Abstract
Introduction: One of the main causes of death in European and US intensive care units is sepsis. It involves a network of pro-inflammatory cytokines such as TNF-alpha, IL-1beta and IL-6. Furthermore, there is an up regulation of transcription factors such as nuclear factor (NF) kappaB. It has previously been shown that clonidine is able to significantly reduce pro-inflammatory cytokines in surgical patients. We therefore hypothesise that the clinically used central alpha-2 agonist clonidine has the ability to improve survival in experimental sepsis by inhibiting the sympathetic tone and consequently inhibiting the pro-inflammatory cytokine release.
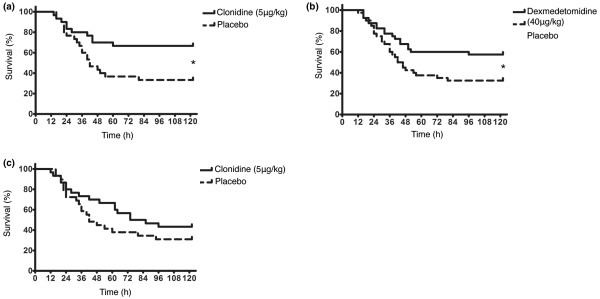
Methods: To investigate this therapeutic potential of clonidine in a prospective randomised laboratory investigation we used a murine model of caecal ligation and puncture (CLP) induced sepsis. Animals receiving pre-emptive injections were treated with either clonidine (5 microg/kg) or dexmedetomidine (40 microg/kg) 12 and 1 hours before the operation, as well as 1, 6 and 12 hours afterwards. Another group of animals only received clonidine (5 microg/kg) 1, 6 and 12 hours after the operation, while the pre-emptive injections were normal saline. The control groups received solvent injections at the respective time points.
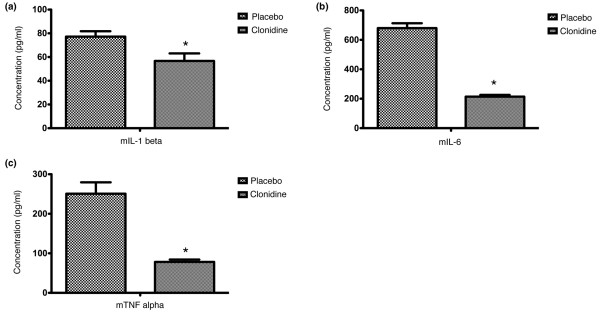
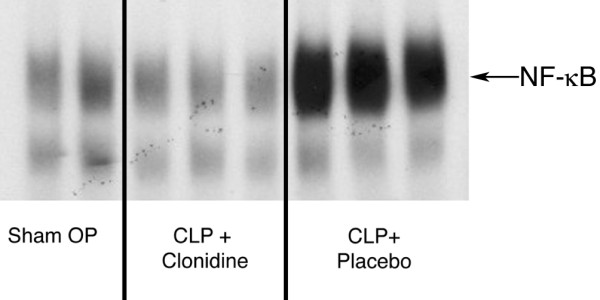
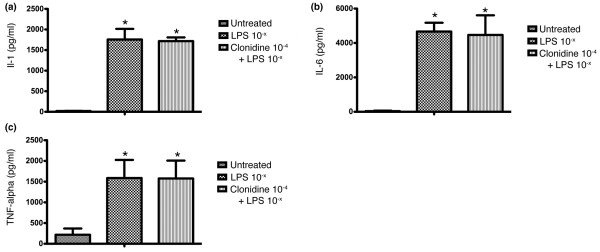
Results: Pre-emptive administration of a central sympatholytic significantly reduced mortality (clonidine: p = 0.015; dexmedetomidine: p = 0.029), although postoperative administration of clonidine failed to significantly prolong survival. Furthermore pre-emptive administration of clonidine significantly attenuated the cytokine response after CLP-induced sepsis (mIL-1beta: p = 0.017; mIL-6: p < 0.0001; mTNF-alpha: p < 0.0001), preserved blood pressure control (p = 0.024) and down-regulated the binding activity of NF-kappaB. There were no changes in the pro-inflammatory cytokine response when peripheral blood was incubated with lipopolysaccharide alone compared with incubation with clonidine (10-4 M) plus LPS (p > 0.05).
Conclusions: Our results demonstrate that the pre-emptive administration of either clonidine or dexmedetomidine have the ability to successfully improve survival in experimental sepsis. Furthermore, there seems to be a connection between the central muscarinic network and the vagal cholinergic response. By down-regulating pro-inflammatory mediators sympatholytics may be a useful adjunct sedative in patients with a high risk for developing sepsis.
Figures
Comment in
-
Neuroimmune perspectives in sepsis.Crit Care. 2009;13(2):133. doi: 10.1186/cc7758. Epub 2009 Apr 23. Crit Care. 2009. PMID: 19439052 Free PMC article.
References
-
- Elia N, Culebras X, Mazza C, Schiffer E, Tramer MR. Clonidine as an adjuvant to intrathecal local anesthetics for surgery: systematic review of randomized trials. Reg Anesth Pain Med. 2008;33:159–167. - PubMed
-
- Alcohol withdrawal syndrome: how to predict, prevent, diagnose and treat it. Prescrire Int. 2007;16:24–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
