

Effect of fish oil on ventricular tachyarrhythmia in three studies in patients with implantable cardioverter defibrillators
- PMID: 19196720
- PMCID: PMC2663728
- DOI: 10.1093/eurheartj/ehp003
Effect of fish oil on ventricular tachyarrhythmia in three studies in patients with implantable cardioverter defibrillators
Abstract
Aims: To determine the effects of omega-3 polyunsaturated fatty acids (omega-3 PUFAs) from fish on the incidence of recurrent ventricular arrhythmia in implantable cardioverter defibrillator (ICD) patients by combining results from published trials.
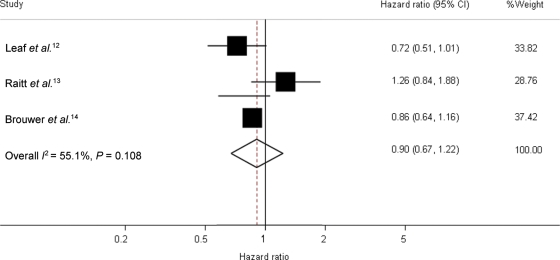
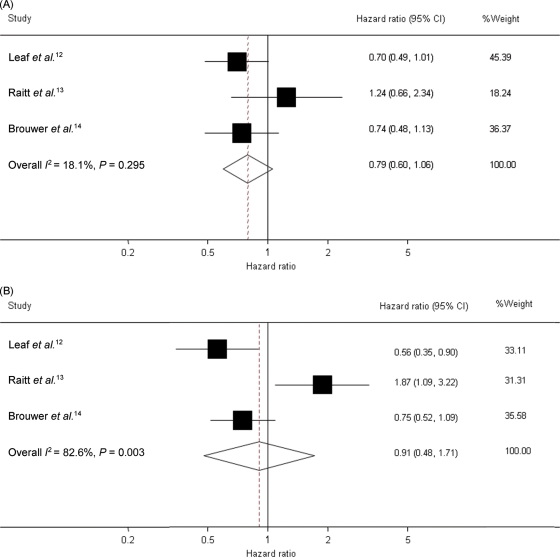
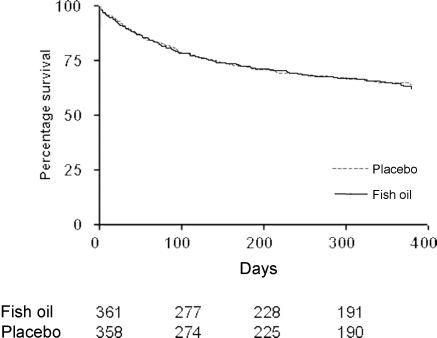
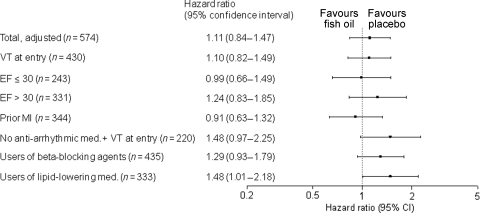
Methods and results: We searched in the Medline, EMBASE, and Cochrane databases and performed a meta-analysis on all three available trials on fish oil and ventricular arrhythmia. Furthermore, we pooled individual data of two of these randomized, double-blind, placebo-controlled trials (Raitt et al. Fish oil supplementation and risk of ventricular tachycardia and ventricular fibrillation in patients with implantable defibrillators: a randomized controlled trial. JAMA 2005;293:2884-2891 and Brouwer et al. Effect of fish oil on ventricular tachyarrhythmia and death in patients with implantable cardioverter defibrillators: the Study on Omega-3 Fatty Acids and Ventricular Arrhythmia (SOFA) randomized trial. JAMA 2006;295:2613-2619). The main outcome was time to first confirmed ventricular fibrillation (VF) or ventricular tachycardia (VT) combined with death for the meta-analysis, and time to first spontaneous confirmed VF or VT for the pooled analysis. The meta-analysis (n = 1148) showed no convincing protective effect of fish oil (RR 0.90; 95% CI 0.67-1.22). The hazard ratio for the subgroup of patients with coronary artery disease at baseline (0.79; 0.60-1.06) tended towards a protective effect. The pooled analysis (n = 722) showed that time to appropriate ICD intervention was similar for fish oil and placebo treatment (log-rank P = 0.79).
Conclusion: These findings do not support a protective effect of omega-3 PUFAs from fish oil on cardiac arrhythmia in all patients with an ICD. Current data neither prove nor disprove a beneficial or a detrimental effect for subgroups of patients with specific underlying pathologies.
Figures
References
-
- He K, Song Y, Daviglus ML, Liu K, Van Horn L, Dyer AR, Greenland P. Accumulated evidence on fish consumption and coronary heart disease mortality: a meta-analysis of cohort studies. Circulation. 2004;109:2705–2711. - PubMed
-
- Whelton SP, He J, Whelton PK, Muntner P. Meta-analysis of observational studies on fish intake and coronary heart disease. Am J Cardiol. 2004;93:1119–1123. - PubMed
-
- Burr ML, Fehily AM, Gilbert JF, Rogers S, Holliday RM, Sweetnam PM, Elwood PC, Deadman NM. Effects of changes in fat, fish, and fibre intakes on death and myocardial reinfarction: diet and reinfarction trial (DART) Lancet. 1989;2:757–761. - PubMed
-
- Investigators GISSI-Prevenzione. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto miocardico. Lancet. 1999;354:447–455. - PubMed
-
- Siscovick DS, Raghunathan TE, King I, Weinmann S, Wicklund KG, Albright J, Bovbjerg V, Arbogast P, Smith H, Kushi LH, Cobb LA, Copass MK, Psaty BM, Lemaitre R, Retzlaff B, Childs M, Knopp RH. Dietary intake and cell membrane levels of long-chain n-3 polyunsaturated fatty acids and the risk of primary cardiac arrest. JAMA. 1995;274:1363–1367. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
