

Increased xanthine oxidase in the skin of preeclamptic women
- PMID: 19196876
- PMCID: PMC2992872
- DOI: 10.1177/1933719108329817
Increased xanthine oxidase in the skin of preeclamptic women
Abstract
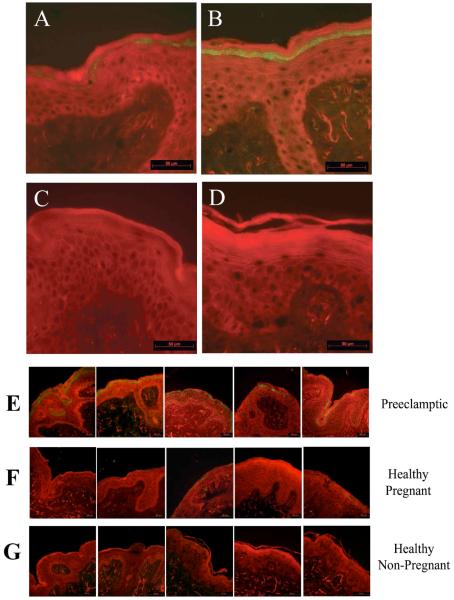
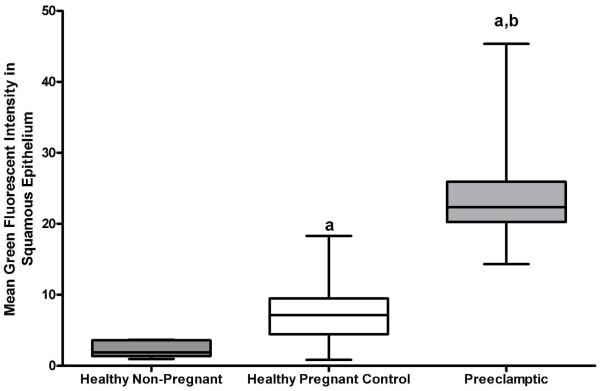
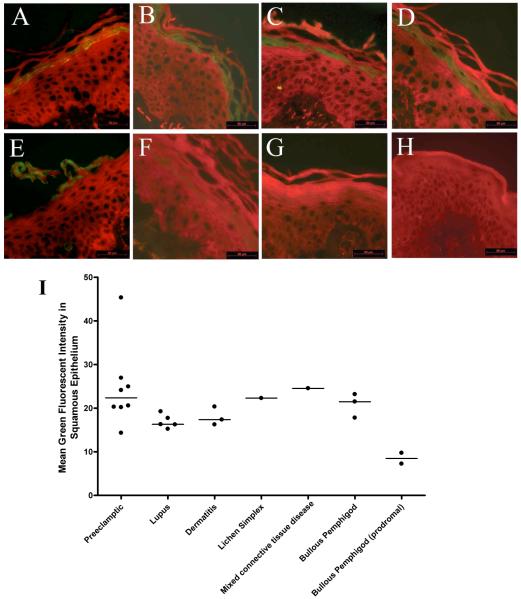
Xanthine oxioreductase is the holoenzyme responsible for terminal purine catabolism. Under conditions of metabolic stress or heightened proinflammatory cytokine production, this enzyme is preferentially in its oxidized form, xanthine oxidase, with catalytic action that generates uric acid and the free radical superoxide. As preeclampsia is characterized by heightened inflammation, oxidative stress, and hyperuricemia, it has been proposed that xanthine oxidase plays a pivotal role in this hypertensive disorder of pregnancy. We sought to determine whether xanthine oxidase protein content was higher in maternal tissue of preeclamptic mothers, compared to healthy pregnant controls, using immunohistochemical analysis of skin biopsies. We further compared xanthine oxidase immunoreactivity in skin biopsies from preeclamptic women and patients with several inflammatory conditions. In preeclamptic women, intense xanthine oxidase immunoreactivity was present within the epidermis. By contrast, only very faint xanthine oxidase staining was observed in skin biopsies from healthy pregnant controls. Further, a role for inflammation in the increase of xanthine oxidase was suggested by similar findings of heightened xanthine oxidase immunoreactivity in the skin biopsies from nonpregnant individuals diagnosed with conditions of systemic inflammation. The finding of increased xanthine oxidase in maternal tissue, most likely as the result of heightened maternal inflammation, suggests maternal xanthine oxidase as a source of free radical and uric acid generation in preeclampsia.
Figures
References
-
- Saito S, Shiozaki A, Nakashima A, Sakai M, Sasaki Y. The role of the immune system in preeclampsia. Mol Aspects Med. 2007 Apr;28(2):192–209. - PubMed
-
- Walther T, Wallukat G, Jank A, et al. Angiotensin II type 1 receptor agonistic antibodies reflect fundamental alterations in the uteroplacental vasculature. Hypertension. 2005 Dec;46(6):1275–1279. - PubMed
-
- Qiu C, Luthy DA, Zhang C, Walsh SW, Leisenring WM, Williams MA. A prospective study of maternal serum C-reactive protein concentrations and risk of preeclampsia. Am J Hypertens. 2004 Feb;17(2):154–160. - PubMed
-
- Powers RW, Bodnar LM, Ness RB, et al. Uric acid concentrations in early pregnancy among preeclamptic women with gestational hyperuricemia at delivery. Am J Obstet Gynecol. 2006 Jan;194(1):160. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
