

Effects of type 2 diabetes on insulin secretion, insulin action, glucose effectiveness, and postprandial glucose metabolism
- PMID: 19196896
- PMCID: PMC2671126
- DOI: 10.2337/dc08-1826
Effects of type 2 diabetes on insulin secretion, insulin action, glucose effectiveness, and postprandial glucose metabolism
Abstract
Objective: In this study, we sought to determine whether postprandial insulin secretion, insulin action, glucose effectiveness, and glucose turnover were abnormal in type 2 diabetes.
Research design and methods: Fourteen subjects with type 2 diabetes and 11 nondiabetic subjects matched for age, weight, and BMI underwent a mixed-meal test using the triple-tracer technique. Indexes of insulin secretion, insulin action, and glucose effectiveness were assessed using the oral "minimal" and C-peptide models.
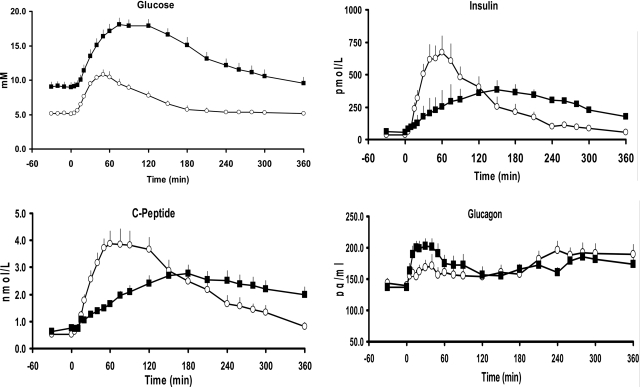
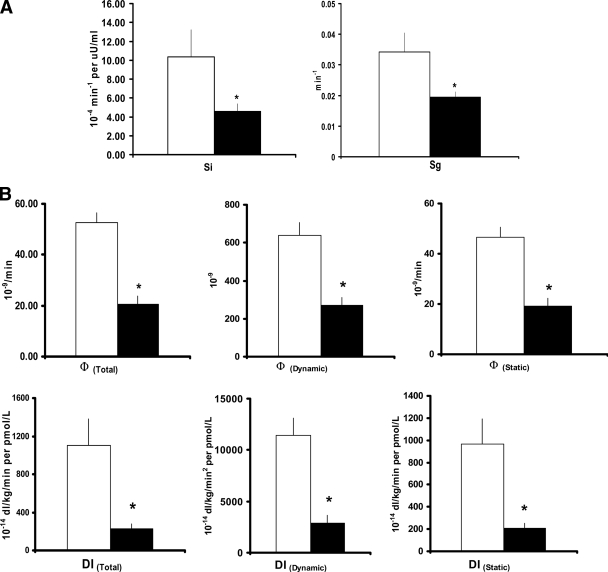
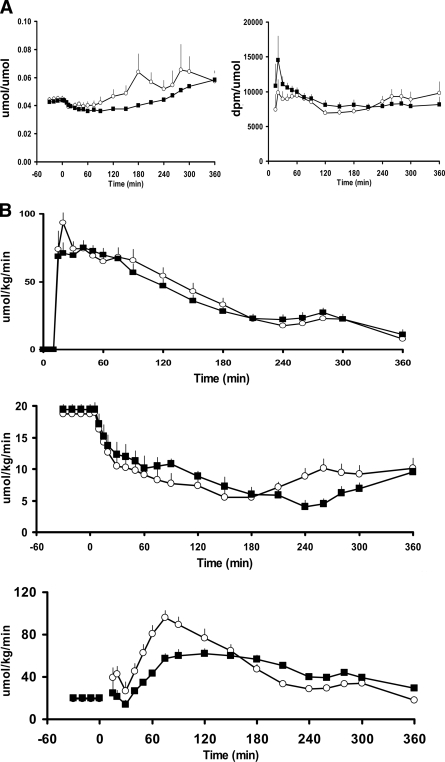
Results: Fasting and postprandial glucose concentrations were higher in the diabetic than nondiabetic subjects. Although peak insulin secretion was delayed (P < 0.001) and lower (P < 0.05) in type 2 diabetes, the integrated total postprandial insulin response did not differ between groups. Insulin action, insulin secretion, disposition indexes, and glucose effectiveness all were lower (P < 0.05) in diabetic than in nondiabetic subjects. Whereas the rate of meal glucose appearance did not differ between groups, the percent suppression of endogenous glucose production (EGP) was slightly delayed and the increment in glucose disappearance was substantially lower (P < 0.01) in diabetic subjects during the first 3 h after meal ingestion. Together, these defects resulted in an excessive rise in postprandial glucose concentrations in the diabetic subjects.
Conclusions: When measured using methods that avoid non-steady-state error, the rate of appearance of ingested glucose was normal and suppression of EGP was only minimally impaired. However, when considered in light of the prevailing glucose concentration, both were abnormal. In contrast, rates of postprandial glucose disappearance were substantially decreased due to defects in insulin secretion, insulin action, and glucose effectiveness.
Figures
References
-
- Basu R, Schwenk WF, Rizza RA: Both fasting glucose production and disappearance are abnormal in people with “mild” and “severe” type 2 diabetes. Am J Physiol Endocrinol Metab 2004; 287: E55– E62 - PubMed
-
- Boden G, Chen X, Stein TP: Gluconeogenesis in moderately and severely hyperglycemic patients with type 2 diabetes mellitus. Am J Physiol Endocrinol Metab 2001; 280: E23– E30 - PubMed
-
- DeFronzo RA, Ferrannini E, Simonson DC: Fasting hyperglycemia in non-insulin-dependent diabetes mellitus: contributions of excessive hepatic glucose production and impaired tissue glucose uptake. Metabolism 1989; 38: 387– 395 - PubMed
-
- Ferrannini E, Simonson DC, Katz LD, Reichard G, Jr, Bevilacqua S, Barrett EJ, Olsson M, DeFronzo RA: The disposal of an oral glucose load in patients with non-insulin-dependent diabetes. Metabolism 1988; 37: 79– 85 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
