

Prognostic gene signatures for non-small-cell lung cancer
- PMID: 19196983
- PMCID: PMC2636731
- DOI: 10.1073/pnas.0809444106
Prognostic gene signatures for non-small-cell lung cancer
Abstract
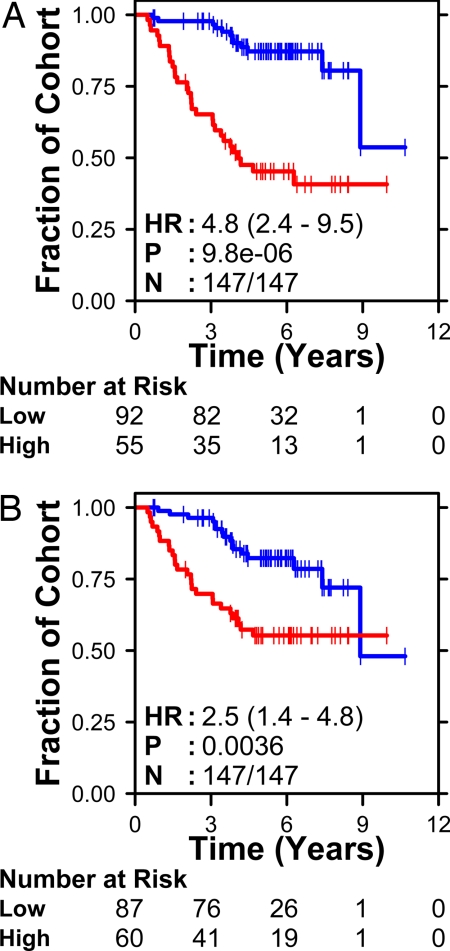
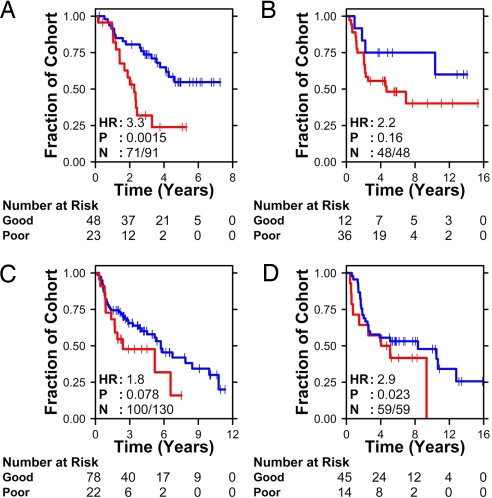
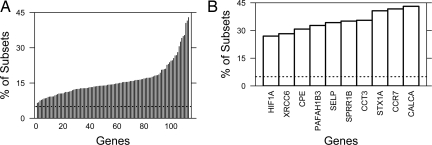
Resectable non-small-cell lung cancer (NSCLC) patients have poor prognosis, with 30-50% relapsing within 5 years. Current staging criteria do not fully capture the complexity of this disease. Survival could be improved by identification of those early-stage patients who are most likely to benefit from adjuvant therapy. Molecular classification by using mRNA expression profiles has led to multiple, poorly overlapping signatures. We hypothesized that differing statistical methodologies contribute to this lack of overlap. To test this hypothesis, we analyzed our previously published quantitative RT-PCR dataset with a semisupervised method. A 6-gene signature was identified and validated in 4 independent public microarray datasets that represent a range of tumor histologies and stages. This result demonstrated that at least 2 prognostic signatures can be derived from this single dataset. We next estimated the total number of prognostic signatures in this dataset with a 10-million-signature permutation study. Our 6-gene signature was among the top 0.02% of signatures with maximum verifiability, reaffirming its efficacy. Importantly, this analysis identified 1,789 unique signatures, implying that our dataset contains >500,000 verifiable prognostic signatures for NSCLC. This result appears to rationalize the observed lack of overlap among reported NSCLC prognostic signatures.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Tsuboi M, et al. The present status of postoperative adjuvant chemotherapy for completely resected non-small cell lung cancer. Ann Thorac Cardiovasc Surg. 2007;13:73–77. - PubMed
-
- Mountain CF. Staging classification of lung cancer. A critical evaluation. Clin Chest Med. 2002;23:103–121. - PubMed
-
- Mountain CF. Revisions in the International System for Staging Lung Cancer. Chest. 1997;111:1710–1717. - PubMed
-
- Jones KL, Buzdar AU. A review of adjuvant hormonal therapy in breast cancer. Endocr Relat Cancer. 2004;11:391–406. - PubMed
-
- Zaniboni A, Labianca R. Adjuvant therapy for stage II colon cancer: An elephant in the living room? Ann Oncol. 2004;15:1310–1318. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
