

Hypofractionation for prostate cancer
- PMID: 19197165
- PMCID: PMC3039916
- DOI: 10.1097/PPO.0b013e3181976614
Hypofractionation for prostate cancer
Abstract
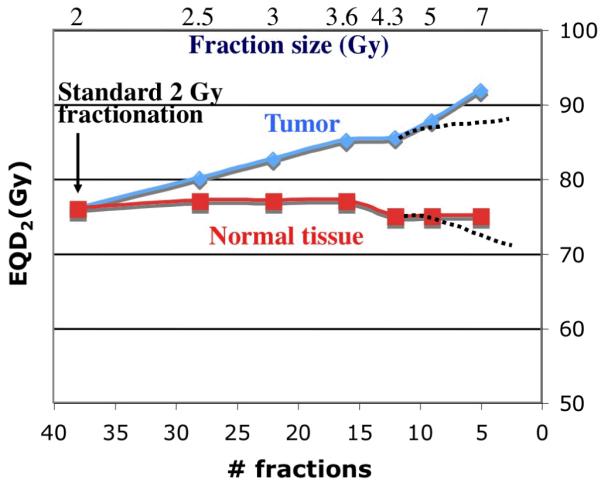
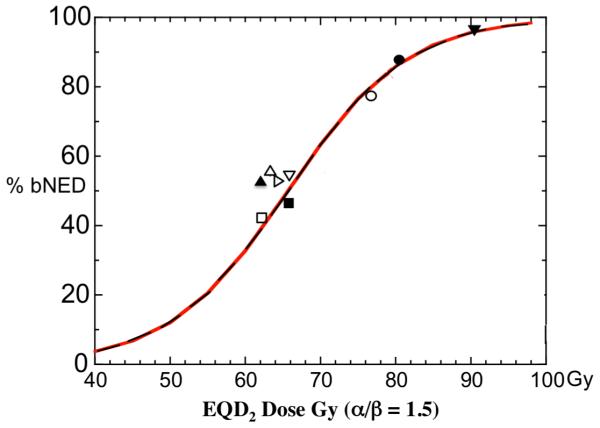
Hypofractionation for prostate cancer was originally carried out in the pursuit of efficiency and convenience but has now attracted greatly renewed interest based upon a hypothesis that prostate cancers have a higher sensitivity to fraction size, reflected in a low alpha/beta ratio, than do late responding organs at risk such as the rectum or bladder. Tumor control and acceptable toxicity outcomes from several hypofractionation or brachytherapy analyses do in fact support an alpha/beta ratio for prostate cancer that is low, perhaps even lower that that for the normal organs that ordinarily constrain the delivery of radiation therapy. However, many of these studies lack sufficient patient numbers and follow-up, are clouded by dose inhomogeneity issues in the case of brachytherapy, or delivered effective doses that were too low by contemporary standards. Thus, the clinical efficacy of the approach has yet to be fully validated. However, a number of newer prospective trials, some randomized, are underway or have reached accrual but await sufficient follow-up for analysis. These studies, which cover a wide range of doses per fraction, should ultimately be capable of validating the utility of prostate hypofractionation and the models that predict its effects. With hypofractionation's significant potential for therapeutic gain, cost savings, and improved patient convenience, the future management of localized prostate cancer could be profoundly altered in the process.
Figures
References
-
- Bentzen SM, Overgaard J, Thames HD, et al. Clinical radiobiology of malignant melanoma. Radiother Oncol. 1989;16:169–182. - PubMed
-
- Thames HD, Suit HD. Tumor radioresponsiveness versus fractionation sensitivity. Int J Radiat Oncol Biol Phys. 1986;12:687–691. - PubMed
-
- Haustermans KM, Hofland I, VP H, et al. Cell kinetic measurements in prostate cancer. Int J Radiat Oncol Biol Phys. 1997;37:1067–1070. - PubMed
-
- Pollack A, Zagars GK, Kavadi VS. Prostate specific antigen doubling time and disease relapse after radiotherapy for prostate cancer. Cancer. 1994;74:670–678. - PubMed
-
- Brenner DJ, Hall EJ. Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys. 1999;43:1095–1101. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
