

Clinical significance of tumor markers and an emerging perspective on colorectal cancer
- PMID: 19200256
- PMCID: PMC11158403
- DOI: 10.1111/j.1349-7006.2008.01022.x
Clinical significance of tumor markers and an emerging perspective on colorectal cancer
Abstract
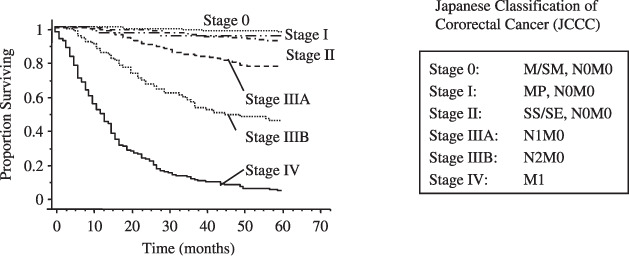
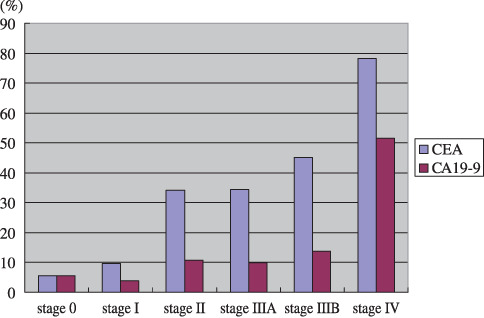
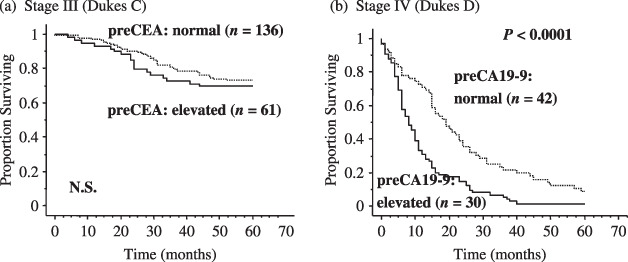
Serum carcinoembryonic antigen (CEA) and CA19-9, a carbohydrate antigen recognized by the monoclonal antibody NS19-9, are commonly used as classical tumor markers in colorectal cancer (CRC) clinics. The roles of tumor markers include: (1) diagnostic screening (diagnostic markers); (2) prediction of prognosis after treatment (prognostic markers); and (3) judgment tools for treatment effect (surveillance markers). Tumor markers can be evaluated in serum, stools, or even in tissues depending on the clinical purpose. The American Society for Clinical Oncology recommends that CEA is the only marker of choice for monitoring the response of metastatic disease to systemic therapy at present. In the present paper, we are the first to review the clinical significance of the classical tumor markers CEA and CA19-9 in serum, allowing for our original data, and present our view on the newly emerging biomarkers in CRC. Novel promising biomarkers for diagnostic, prognostic, and surveillance purposes are reviewed and considered, some of which are anticipated for further validation. For diagnostic markers, urine or serum might replace fecal samples in the near future. On the other hand, prognostic or predictive markers for treatment sensitivity may be identified from the molecular profiles of primary cancer tissues. Selection of patients who are sensitive to chemotherapy will reduce the number of patients who undergo harmful chemotherapy with no effectiveness. The optimal tumor markers would be generalized, easy to assess, and accurate, and such markers are eagerly anticipated to enable personalized tailored therapy for CRC patients.
Figures
References
-
- Mandel JS, Bond JH, Church TR et al . Reducing mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med 1993; 328: 1365–71. - PubMed
-
- Mandel JS, Church TR, Ederer F et al . Colorectal cancer mortality: effectiveness of biennial screening for fecal occult blood. J Natl Cancer Inst 1999; 91: 434–7. - PubMed
-
- Kronborg O, Fenger C, Olsen J et al . Randomised study of screening for colorectal cancer with fecal‐occult‐blood test. Lancet 1996; 348: 1467–71. - PubMed
-
- Hardcastle JD, Chamberlain JO, Robinson MHE et al . Randomised controlled trial of fecal‐occult‐blood screening for colorectal cancer. Lancet 1996; 348: 1472–7. - PubMed
-
- Sonnenberg A, Delco F, Inadomi JM. Cost‐effectiveness of colonoscopy in screening for colorectal cancer. Ann Intern Med 2000; 133: 573–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
