

Cell therapy with bone marrow cells for myocardial regeneration
- PMID: 19203213
- PMCID: PMC2788115
- DOI: 10.1089/ars.2009.2486
Cell therapy with bone marrow cells for myocardial regeneration
Abstract
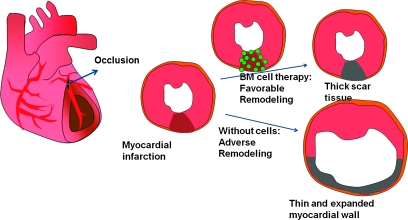
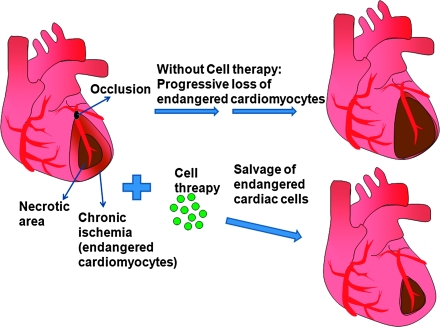
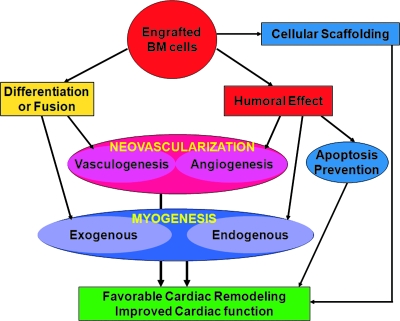
Cell therapy has tremendous potential for the damaged heart, which has limited self-renewing capability. Bone marrow (BM) cells are attractive for cell therapy, as they contain diverse stem and progenitor cell populations that can give rise to various cell types, including cardiomyocytes, endothelial cells, and smooth muscle cells. Studies have shown BM cells to be safe and efficacious in the treatment of myocardial infarction. Possible therapeutic mechanisms mediated by both host and transplanted cells include cardiomyogenesis, neovascularization, and attenuation of adverse remodeling. In this review, different stem and progenitor cells in the bone marrow and their application in cell therapy are reviewed, and evidence for their therapeutic mechanisms is discussed.
Figures
Similar articles
-
Myocardial regeneration with bone-marrow-derived stem cells.Biol Cell. 2005 Apr;97(4):253-63. doi: 10.1042/BC20040099. Biol Cell. 2005. PMID: 15762847 Review.
-
Clonally expanded novel multipotent stem cells from human bone marrow regenerate myocardium after myocardial infarction.J Clin Invest. 2005 Feb;115(2):326-38. doi: 10.1172/JCI22326. J Clin Invest. 2005. PMID: 15690083 Free PMC article.
-
Stem cell therapy for acute myocardial infarction - focusing on the comparison between Muse cells and mesenchymal stem cells.J Cardiol. 2022 Jul;80(1):80-87. doi: 10.1016/j.jjcc.2021.10.030. Epub 2021 Dec 17. J Cardiol. 2022. PMID: 34924234 Review.
-
Autologous bone marrow-derived progenitor cell transplantation for myocardial regeneration after acute infarction.Vojnosanit Pregl. 2004 Sep-Oct;61(5):519-29. doi: 10.2298/vsp0405519o. Vojnosanit Pregl. 2004. PMID: 15551805
-
Neovascularization and cardiomyocytes regeneration in acute myocardial infarction after bone marrow stromal cell transplantation: comparison of infarct-relative and noninfarct-relative arterial approaches in swine.Clin Chim Acta. 2007 Jun;381(2):114-8. doi: 10.1016/j.cca.2007.02.035. Epub 2007 Feb 23. Clin Chim Acta. 2007. PMID: 17400203
Cited by
-
Emerging therapy for diabetic neuropathy: cell therapy targeting vessels and nerves.Endocr Metab Immune Disord Drug Targets. 2012 Jun;12(2):168-78. doi: 10.2174/187153012800493486. Endocr Metab Immune Disord Drug Targets. 2012. PMID: 22236028 Free PMC article. Review.
-
Identification of a coronary stem cell in the human heart.J Mol Med (Berl). 2011 Oct;89(10):947-59. doi: 10.1007/s00109-011-0769-8. Epub 2011 May 24. J Mol Med (Berl). 2011. PMID: 21607542 Free PMC article. Review.
-
Stem cells in the diabetic infarcted heart.Heart Fail Rev. 2010 Nov;15(6):581-8. doi: 10.1007/s10741-010-9172-8. Heart Fail Rev. 2010. PMID: 20559720 Free PMC article. Review.
-
Discrepancy between short-term and long-term effects of bone marrow-derived cell therapy in acute myocardial infarction: a systematic review and meta-analysis.Stem Cell Res Ther. 2016 Oct 20;7(1):153. doi: 10.1186/s13287-016-0415-z. Stem Cell Res Ther. 2016. PMID: 27765070 Free PMC article.
-
Adrenomedullin as a growth and cell fate regulatory factor for adult neural stem cells.Stem Cells Int. 2012;2012:804717. doi: 10.1155/2012/804717. Epub 2012 Sep 24. Stem Cells Int. 2012. PMID: 23049570 Free PMC article.
References
-
- Abbate A. Bussani R. Biondi-Zoccai GG. Rossiello R. Silvestri F. Baldi F. Biasucci LM. Baldi A. Persistent infarct-related artery occlusion is associated with an increased myocardial apoptosis at postmortem examination in humans late after an acute myocardial infarction. Circulation. 2002;106:1051–1054. - PubMed
-
- Alvarez-Dolado M. Pardal R. Garcia-Verdugo JM. Fike JR. Lee HO. Pfeffer K. Lois C. Morrison SJ. Alvarez-Buylla A. Fusion of bone-marrow-derived cells with Purkinje neurons, cardiomyocytes and hepatocytes. Nature. 2003;425:968–973. - PubMed
-
- Amado LC. Saliaris AP. Schuleri KH. St John M. Xie JS. Cattaneo S. Durand DJ. Fitton T. Kuang JQ. Stewart G. Lehrke S. Baumgartner WW. Martin BJ. Heldman AW. Hare JM. Cardiac repair with intramyocardial injection of allogeneic mesenchymal stem cells after myocardial infarction. Proc Natl Acad Sci U S A. 2005;102:11474–11479. - PMC - PubMed
-
- Asahara T. Masuda H. Takahashi T. Kalka C. Pastore C. Silver M. Kearne M. Magner M. Isner JM. Bone marrow origin of endothelial progenitor cells responsible for postnatal vasculogenesis in physiological and pathological neovascularization. Circ Res. 1999;85:221–228. - PubMed
-
- Asahara T. Murohara T. Sullivan A. Silver M. van der Zee R. Li T. Witzenbichler B. Schatteman G. Isner JM. Isolation of putative progenitor endothelial cells for angiogenesis. Science. 1997;275:964–967. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
