

Follicular lymphoma in the United States: first report of the national LymphoCare study
- PMID: 19204203
- PMCID: PMC2738614
- DOI: 10.1200/JCO.2008.18.1495
Follicular lymphoma in the United States: first report of the national LymphoCare study
Abstract
Purpose: Optimal therapy of follicular lymphoma (FL) is not defined. We analyzed a large prospective cohort study to identify current demographics and patterns of care of FL in the United States.
Patients and methods: The National LymphoCare Study is a multicenter, longitudinal, observational study designed to collect information on treatment regimens and outcomes for patients with newly diagnosed FL in the United States. Patients were enrolled between 2004 and 2007. There is no study-specific prescribed treatment regimen or intervention.
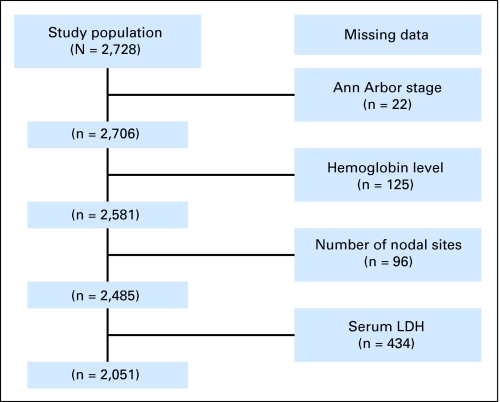
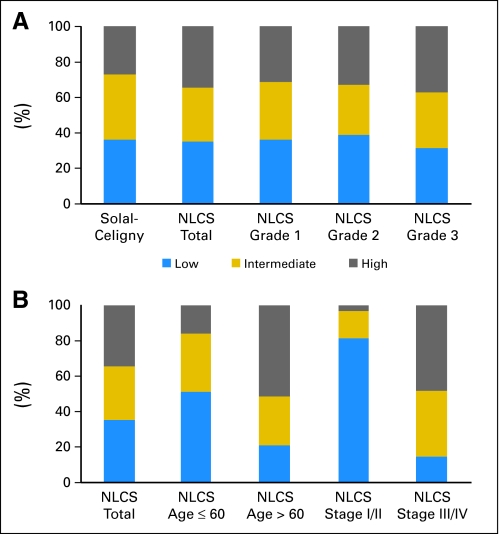
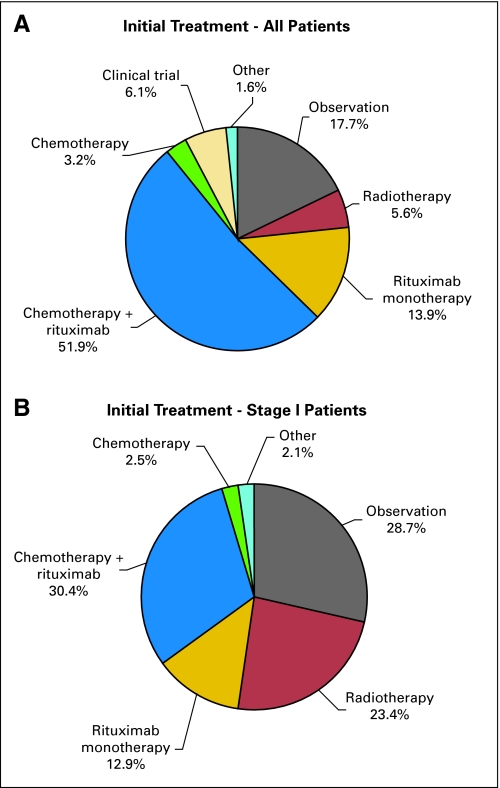
Results: Two thousand seven hundred twenty-eight subjects were enrolled at 265 sites, including the 80% of patients enrolled from nonacademic sites. Using the Follicular Lymphoma International Prognostic Index (FLIPI), three distinct groups independent of histologic grade could be defined. Initial therapeutic strategy was: observation, 17.7%; rituximab monotherapy, 13.9%; clinical trial 6.1%; radiation therapy, 5.6%; chemotherapy only, 3.2%; chemotherapy plus rituximab, 51.9%. Chemotherapy plus rituximab regimens were: rituximab plus cyclophosphamide, doxorubicin, vincristine, prednisone, 55.0%; rituximab plus cyclophosphamide, vincristine, and prednisone, 23.1%; rituximab plus fludarabine based, 15.5%; other, 6.4%. The choice to initiate therapy rather than observe was associated with age, FLIPI, stage, and grade (P < .01). Significant differences in treatment (P < .01) across regions of the United States were noted. Contrary to practice guidelines, treatment of stage I FL frequently omits radiation therapy.
Conclusion: Widely disparate therapeutic approaches are utilized for FL. Initial therapy is deferred in a small subset of patients. There is no single standard of care for the treatment of de novo FL, although antibody use is ubiquitous when therapy is initiated. These disparate approaches to the initial care of patients with FL render a heterogeneous group of patients at relapse.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

Comment in
-
A look in the mirror.J Clin Oncol. 2009 Mar 10;27(8):1158-9. doi: 10.1200/JCO.2009.19.8655. Epub 2009 Feb 9. J Clin Oncol. 2009. PMID: 19204191 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Anderson JR, Armitage JO, Weisenburger DD. Epidemiology of the non-Hodgkin's lymphomas: Distributions of the major subtypes differ by geographic locations. Non-Hodgkin's Lymphoma Classification Project. Ann Oncol. 1998;9:717–720. - PubMed
-
- Swenson WT, Wooldridge JE, Lynch CF, et al. Improved survival of follicular lymphoma patients in the United States. J Clin Oncol. 2005;23:5019–5026. - PubMed
-
- Fisher RI, LeBlanc M, Press OW, et al. New treatment options have changed the survival of patients with follicular lymphoma. J Clin Oncol. 2005;23:8447–8452. - PubMed
-
- Liu Q, Fayad L, Cabanillas F, et al. Improvement of overall and failure-free survival in stage IV follicular lymphoma: 25 years of treatment experience at The University of Texas M.D. Anderson Cancer Center. J Clin Oncol. 2006;24:1582–1589. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
