

Exercise dose and quality of life: a randomized controlled trial
- PMID: 19204218
- PMCID: PMC2745102
- DOI: 10.1001/archinternmed.2008.545
Exercise dose and quality of life: a randomized controlled trial
Abstract
Background: Improved quality of life (QOL) is a purported benefit of exercise, but few randomized controlled trials and no dose-response trials have been conducted to examine this assertion.
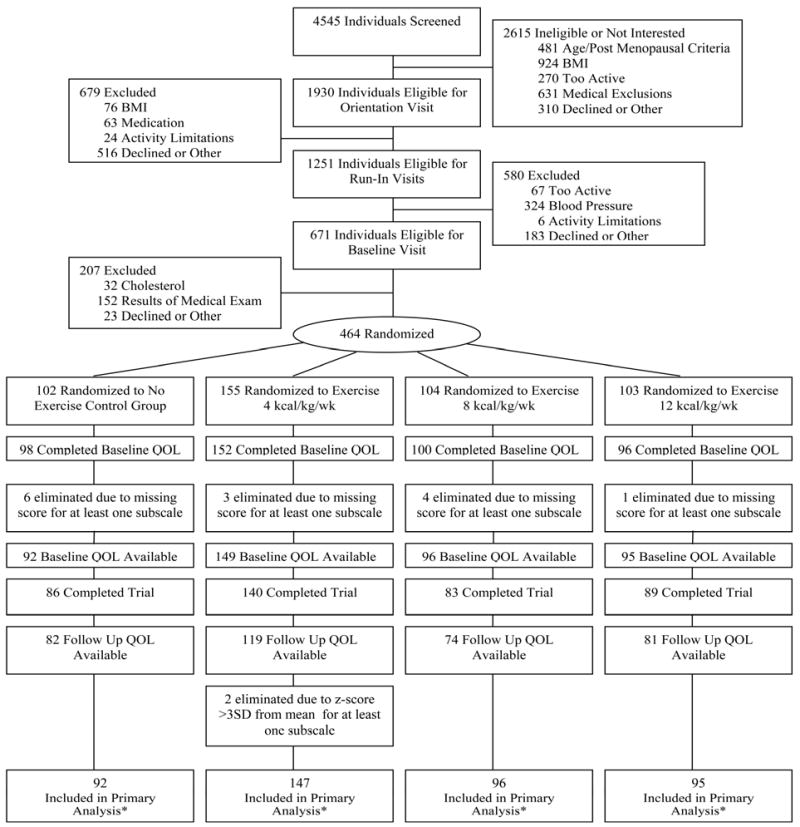
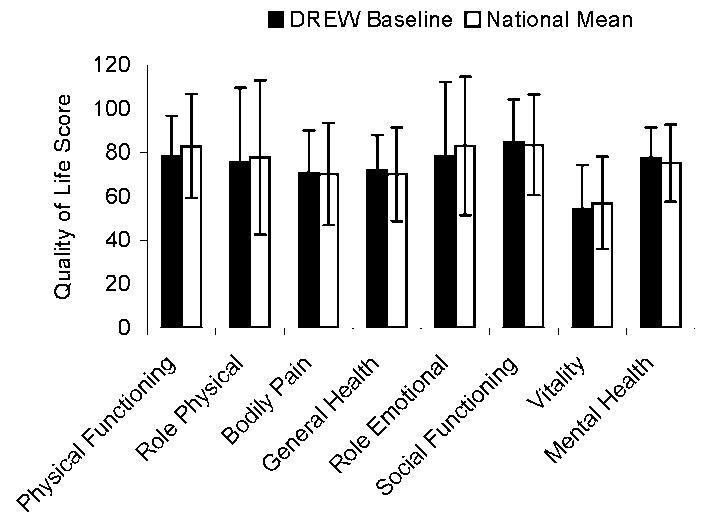
Methods: The effect of 50%, 100%, and 150% of the physical activity recommendation on QOL was examined in a 6-month randomized controlled trial. Participants were 430 sedentary postmenopausal women (body mass index range, 25.0-43.0 [calculated as weight in kilograms divided by height in meters squared]) with elevated systolic blood pressure randomized to a nonexercise control group (n = 92) or 1 of 3 exercise groups: exercise energy expenditure of 4 (n = 147), 8 (n = 96), or 12 (n = 95) kilocalories per kilogram of body weight per week. Eight aspects of physical and mental QOL were measured at baseline and month 6 with the use of the Medical Outcomes Study 36-Item Short Form Health Survey.
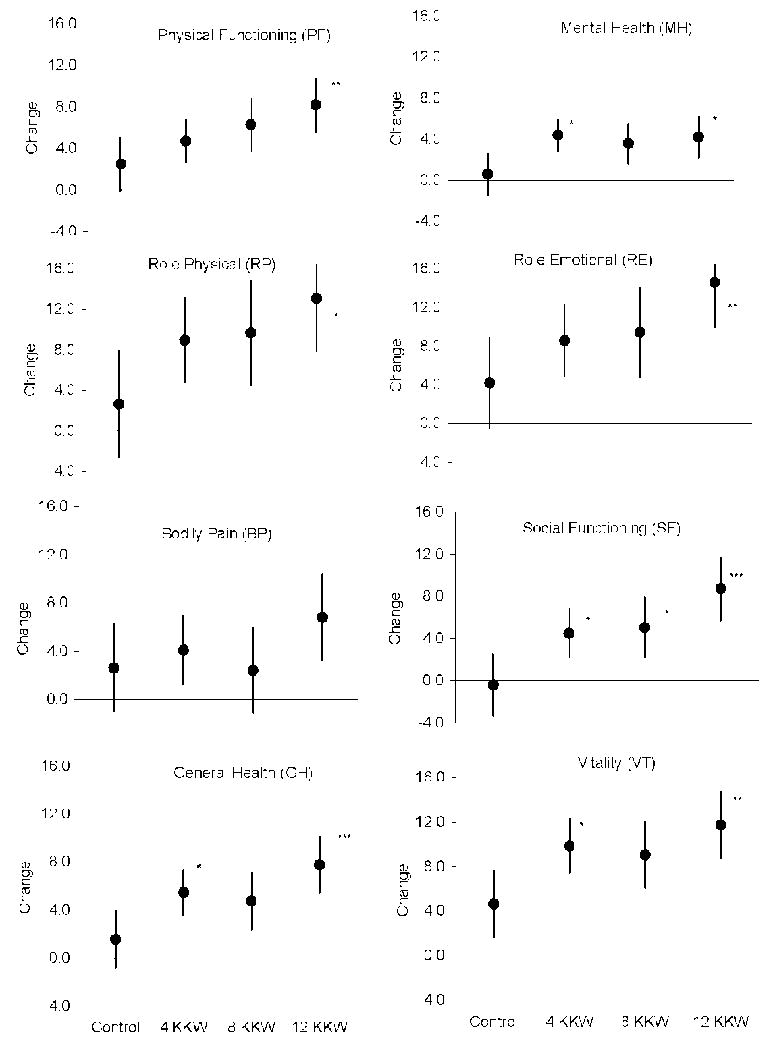
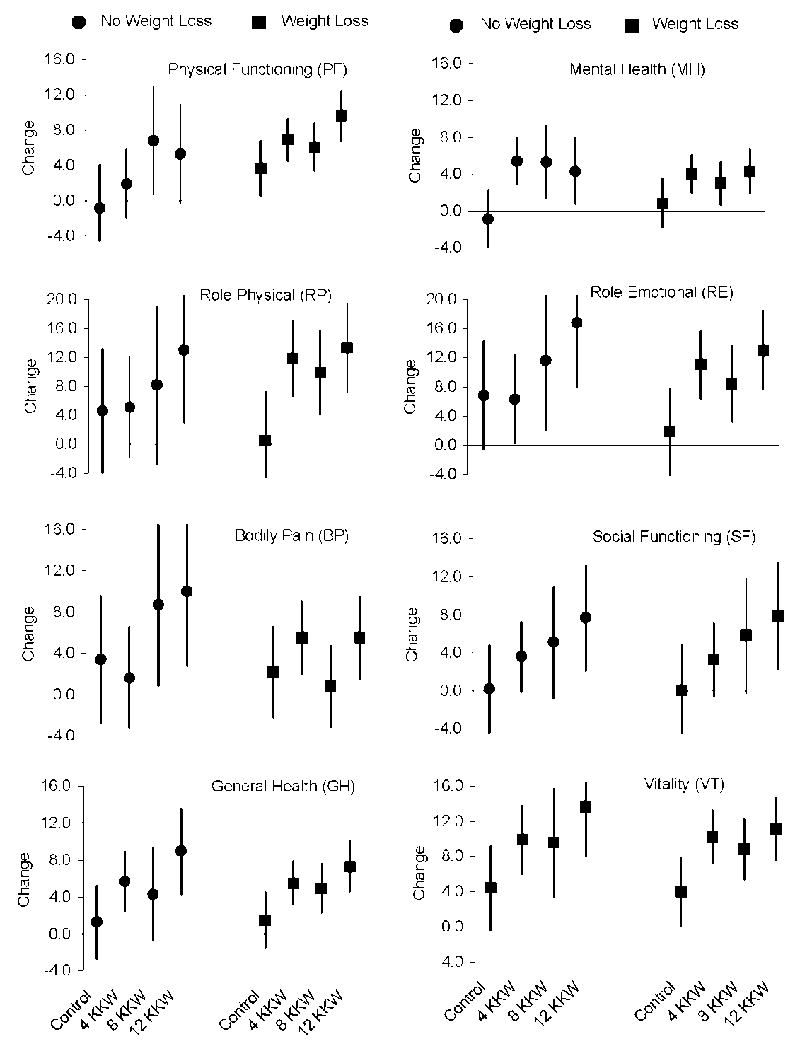
Results: Change in all mental and physical aspects of QOL, except bodily pain, was dose dependent (trend analyses were significant, and exercise dose was a significant predictor of QOL change; P < .05). Higher doses of exercise were associated with larger improvements in mental and physical aspects of QOL. Controlling for weight change did not attenuate the exercise-QOL association.
Conclusion: Exercise-induced QOL improvements were dose dependent and independent of weight change.
Trial registration: ClinicalTrials.gov NCT00011193.
Figures
References
-
- Blair SN, Kohl HW, 3rd, Barlow CE, Paffenbarger RS, Jr, Gibbons LW, Macera CA. Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. JAMA. 1995;273:1093–1098. - PubMed
-
- Blair SN, Kohl HW, 3rd, Paffenbarger RS, Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA. 1989;262:2395–2401. - PubMed
-
- Gulati M, Pandey DK, Arnsdorf MF, et al. Exercise capacity and the risk of death in women: The St James Women Take Heart Project. Circulation. 2003;108:1554–1559. - PubMed
-
- Mora S, Redberg RF, Cui Y, et al. Ability of exercise testing to predict cardiovascular and all-cause death in asymptomatic women: A 20-year follow-up of the lipid research clinics prevalence study. JAMA. 2003;290:1600–1607. - PubMed
-
- Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002;346:793–801. - PubMed
