

Clinical development of new prophylactic antimalarial drugs after the 5th Amendment to the Declaration of Helsinki
- PMID: 19209263
- PMCID: PMC2621393
- DOI: 10.2147/tcrm.s1025
Clinical development of new prophylactic antimalarial drugs after the 5th Amendment to the Declaration of Helsinki
Abstract
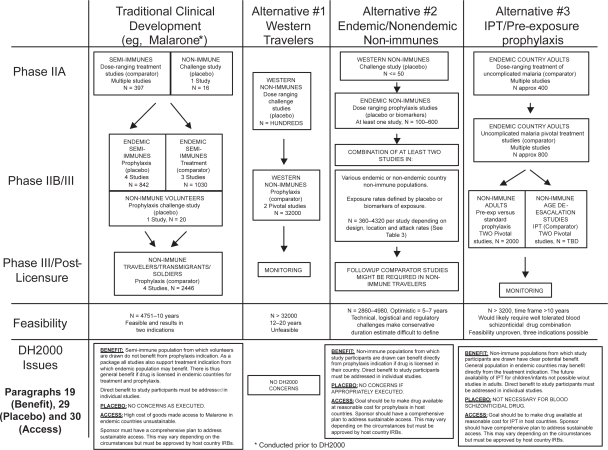
Malaria is of continuing concern in nonimmune traveling populations. Traditionally, antimalarial drugs have been developed as agents for dual indications (treatment and prophylaxis). However, since 2000, when the 5th Amendment to the Declaration of Helsinki (DH2000) was adopted, development of new malaria prophylaxis drugs in this manner has ceased. As a consequence, there may not be any new drugs licensed for this indication in the foreseeable future. Major pharmaceutical companies have interpreted DH2000 to mean that the traditional development paradigm may be considered unethical because of doubt over the likelihood of benefit to endemic populations participating in clinical studies, the use of placebo, and the sustainability of post-trial access to study medications. In this article, we explore the basis of these concerns and suggest that the traditional development paradigm remains ethical under certain circumstances. We also consider alternative approaches that may be more attractive to sponsors as they either do not use placebo, or utilize populations in endemic countries who may unambiguously benefit. These approaches represent the way forward in the future, but are at present unproven in clinical practice, and face numerous regulatory, logistical and technical challenges. Consequently, in the short term, we argue that the traditional clinical development paradigm remains the most feasible approach and is ethical and consistent with the spirit of DH2000 under the appropriate circumstances.
Keywords: DH2000; Declaration of Helsinki; ethics; malaria; prophylaxis; treatment.
Figures
References
-
- Anon Fair benefits for research in developing countries. Science. 2002;298:2133–4. - PubMed
-
- Baird JK, Basri H, Subianto B, et al. Treatment of chloroquine-resistant Plasmodium vivax with chloroquine and primaquine or halofantrine. J Infect Dis. 1995;171:1678–82. - PubMed
-
- Baird JK, Lacey MD, Basri H, et al. Randomized, parallel placebo-controlled trial of primaquine for malaria prophylaxis in Papua, Indonesia. Clin Infect Dis. 2001;22:1990–7. - PubMed
-
- Baird J, Schwartz E, Hoffman S. Prevention and treatment of vivax malaria. Curr Infect Dis Rep. 2007;9:39–46. - PubMed
-
- Bautista CT, Chan AS, Ryan JR, et al. Epidemiology and spatial analysis of malaria in the Northern Peruvian Amazon. Am J Trop Med Hyg. 2006;75:1216–22. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
