

Optimizing prophylactic treatment of migraine: Subtypes and patient matching
- PMID: 19209286
- PMCID: PMC2621398
- DOI: 10.2147/tcrm.s3983
Optimizing prophylactic treatment of migraine: Subtypes and patient matching
Abstract
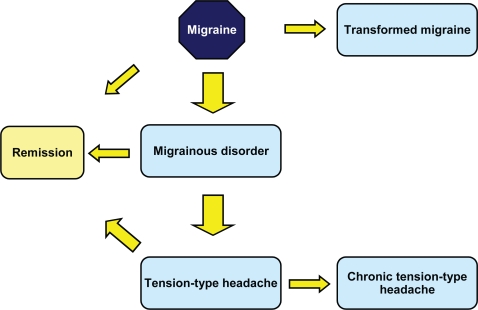
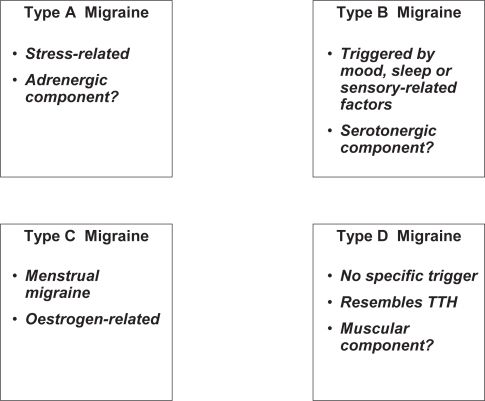
Advances in our understanding of the pathophysiology of migraine have resulted in important breakthroughs in treatment. For example, understanding of the role of serotonin in the cerebrovascular circulation has led to the development of triptans for the acute relief of migraine headaches, and the identification of cortical spreading depression as an early central event associated wih migraine has brought renewed interest in antiepileptic drugs for migraine prophylaxis. However, migraine still remains inadequately treated. Indeed, it is apparent that migraine is not a single disease but rather a syndrome that can manifest itself in a variety of pathological conditions. The consequences of this may be that treatment needs to be matched to particular patients. Clinical research needs to be devoted to identifying which sort of patients benefit best from which treatments, particularly in the field of prophylaxis. We propose four patterns of precipitating factors (adrenergic, serotoninergic, menstrual, and muscular) which may be used to structure migraine prophylaxis. Finally, little is known about long-term outcome in treated migraine. It is possible that appropriate early prophylaxis may modify the long-term course of the disease and avoid late complications.
Keywords: diagnosis; migraine; prophylaxis; subtypes; treatment.
Figures



Similar articles
-
Prophylaxis of menstrual migraine with triptans: problems and possibilities.Neurology. 2002 Dec 10;59(11):1677-81. doi: 10.1212/01.wnl.0000034179.17926.2d. Neurology. 2002. PMID: 12481795 Review.
-
Animal models of migraine headache and aura.Curr Opin Neurol. 2008 Jun;21(3):294-300. doi: 10.1097/WCO.0b013e3282fc25de. Curr Opin Neurol. 2008. PMID: 18451713 Review.
-
Migraine Prophylaxis and Acute Treatment Patterns Among Commercially Insured Patients in the United States.Headache. 2017 Oct;57(9):1399-1408. doi: 10.1111/head.13157. Epub 2017 Aug 26. Headache. 2017. PMID: 28842990
-
Incidence and determinants of migraine prophylactic medication in the Netherlands.Eur J Clin Pharmacol. 2002 May;58(2):149-55. doi: 10.1007/s00228-002-0443-8. Epub 2002 Apr 5. Eur J Clin Pharmacol. 2002. PMID: 12012149
-
Menstrual Migraine and Treatment Options: Review.Headache. 2017 Feb;57(2):194-208. doi: 10.1111/head.12978. Epub 2016 Dec 2. Headache. 2017. PMID: 27910087 Review.
Cited by
-
Comparison of expected outcomes between patients and neurologists using Kano's methodology in symptomatic migraine treatment.Patient. 2012;5(3):147-62. doi: 10.1007/BF03262488. Patient. 2012. PMID: 22506628
References
-
- Adelman LC, Adelman JU, Von Seggern R, et al. Venlafaxine extended release (XR) for the prophylaxis of migraine and tension-type headache: A retrospective study in a clinical setting. Headache. 2000;40:572–80. - PubMed
-
- Adly C, Straumanis J, Chesson A. Fluoxetine prophylaxis of migraine. Headache. 1992;32:101–4. - PubMed
-
- Andersson KE, Vinge E. Beta-adrenoceptor blockers and calcium antagonists in the prophylaxis and treatment of migraine. Drugs. 1990;39:355–73. - PubMed
LinkOut - more resources
Full Text Sources
