

Depressive illness burden associated with complex polypharmacy in patients with bipolar disorder: findings from the STEP-BD
- PMID: 19210946
- PMCID: PMC10034852
- DOI: 10.4088/jcp.08m04301
Depressive illness burden associated with complex polypharmacy in patients with bipolar disorder: findings from the STEP-BD
Abstract
Background: Many patients with bipolar disorder receive multi-drug treatment regimens, but the distinguishing profiles of patients who receive complex pharmacologies have not been established.
Method: Prescribing patterns of lithium, anticonvulsants, antidepressants, and antipsychotics were examined for 4,035 subjects with bipolar disorder (DSM-IV) immediately prior to entering the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). Subjects were recruited for participation across 22 centers in the United States between November 1999 and July 2005. The quality receiver operating characteristic (ROC) method was used to develop composite profiles of patients receiving complex regimens (p < .01 for all iterations).
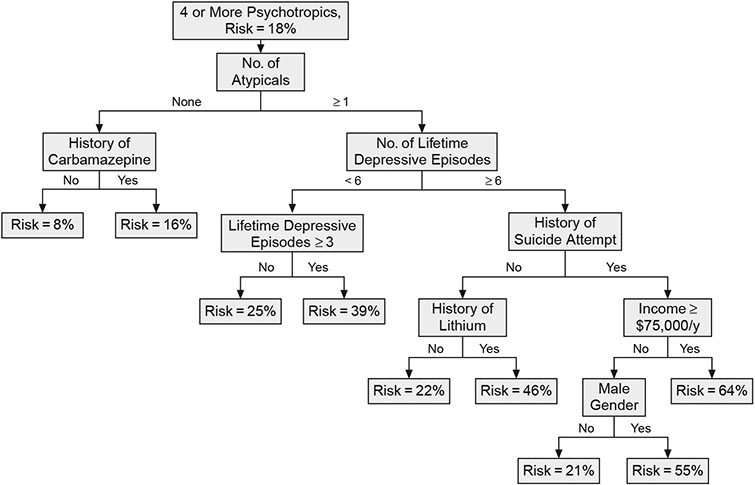
Results: Use of 3 or more medications occurred in 40% of subjects, while 18% received 4 or more agents. Quality ROC analyses revealed that subjects had a 64% risk for receiving a complex regimen (> or = 4 medications) if they had (1) ever taken an atypical antipsychotic, (2) > or = 6 lifetime depressive episodes, (3) attempted suicide, and (4) an annual income > or = $75,000. Complex polypharmacy was least often associated with lithium, divalproex, or carbamazepine and most often associated with atypical antipsychotics or antidepressants. Contrary to expectations, a history of psychosis, age at onset, bipolar I versus II subtype, history of rapid cycling, prior hospitalizations, current illness state, and history of alcohol or substance use disorders did not significantly alter the risk profiles for receiving complex regimens.
Conclusion: Complex polypharmacy involving at least 4 medications occurs in approximately 1 in 5 individuals with bipolar disorder. Use of traditional mood stabilizers is associated with fewer cotherapies. Complex regimens are especially common in patients with substantial depressive illness burden and suicidality, for whom simpler drug regimens may fail to produce acceptable levels of response.
Trial registration: clinicaltrials.gov Identifier: NCT00012558.
Copyright 2009 Physicians Postgraduate Press, Inc.
Figures
References
-
- Frye MA, Ketter TA, Leverich GS, et al. The increasing use of polypharmacotherapy for refractory mood disorders: 22 years of study. J Clin Psychiatry 2000;61(1):9–15 - PubMed
-
- Müller-Oerlinghausen B, Retzow A, Henn FA, et al. Valproate as an adjunct to neuroleptic medication for the treatment of acute episodes of mania: a prospective, randomized, double-blind, placebo-controlled multicenter study. European Valproate Mania Study Group. J Clin Psychopharmacol 2000;20:195–203 - PubMed
-
- Tohen M, Chengappa KN, Suppes T, et al. Efficacy of olanzapine in combination with valproate or lithium in the treatment of mania in patients partially nonresponsive to valproate or lithium monotherapy. Arch Gen Psychiatry 2002;59:62–69 - PubMed
-
- Sachs GS, Grossman F, Ghaemi SN, et al. Combination of a mood stabilizer with risperidone or haloperidol for treatment of acute mania: a double-blind, placebo-controlled comparison of efficacy and safety. Am J Psychiatry 2002;159:1146–1154 - PubMed
-
- Yatham LN, Grossman F, Augustyns I, et al. Mood stabilisers plus risperidone or placebo in the treatment of acute mania: international, double-blind, randomised controlled trial. Br J Psychiatry 2003;182:141–147 - PubMed
