

Perception of risk and knowledge of risk factors in women at high risk for stroke
- PMID: 19211481
- PMCID: PMC2709972
- DOI: 10.1161/STROKEAHA.108.543272
Perception of risk and knowledge of risk factors in women at high risk for stroke
Abstract
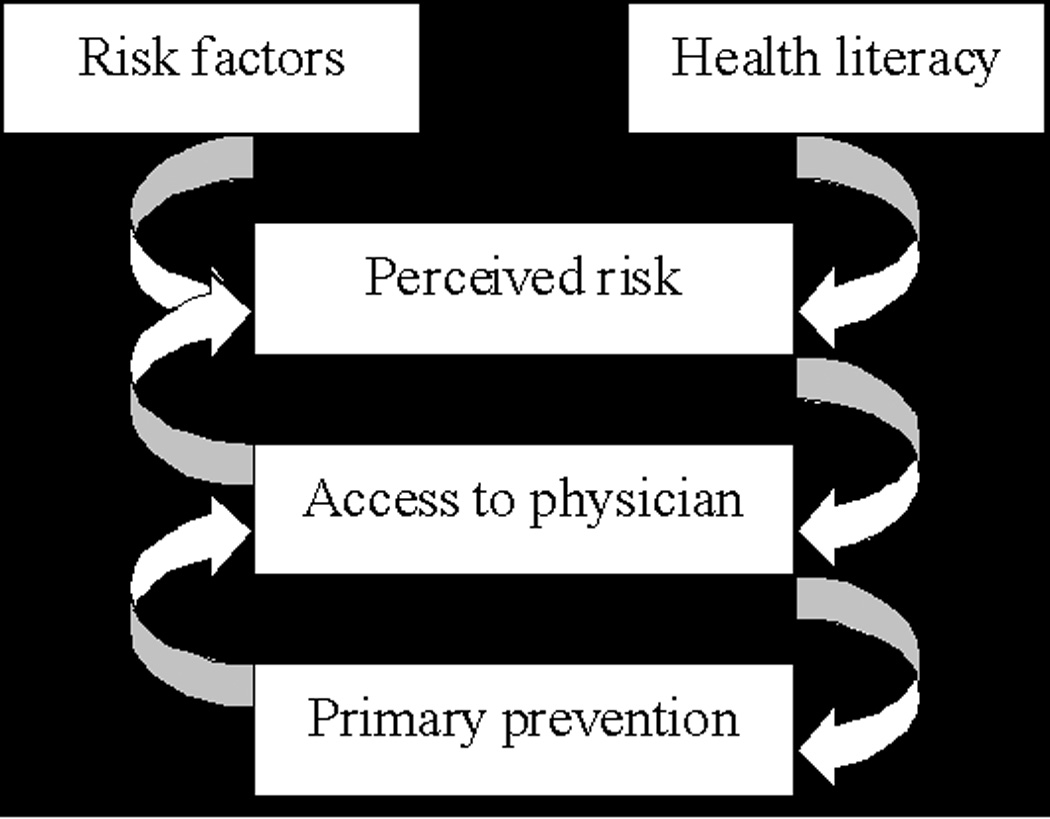
Background and purpose: Women face a higher mortality after stroke and have different risk factors than men. Despite educational campaigns, women continue to underestimate their own risk for stroke. We present a theoretical model to understand risk perception in high-risk women.
Methods: Eight hundred five women, ages 50 to 70 years, were selected from the University of Connecticut Cardiology Center with at least one risk factor for stroke. A 5-part questionnaire addressed stroke knowledge, risk perception, risk factors, access to health care, and demographics. Two hundred fifteen women responded by mail (28% response rate) and deidentified data were entered in SPSS. Descriptive, bivariate, and multivariate techniques assessed the proposed model.
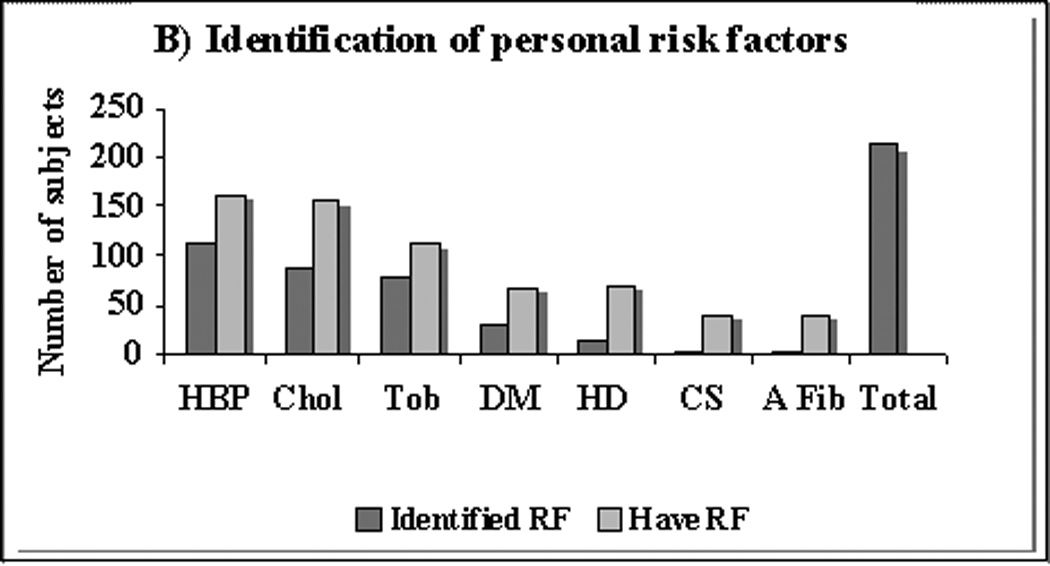
Results: The cohort was predominantly white (91.5%), higher income (33.1% of the population earned >$75,000), and well-educated (28.6% attended graduate or professional school). Only 2 of the 37 (5.4%) women with atrial fibrillation and 11 of the 71 women with heart disease (15.5%) identified their health condition as a risk factor for stroke. Predictors of risk perception included: other women's risk (B=0.336, P<0.001), worrying about stroke (B=0.734, P<0.001), having hypertension (B=0.686, P=0.037), and having diabetes (B=0.893, P=0.004). Only 63.9% of women with atrial fibrillation (n=23) reported taking warfarin.
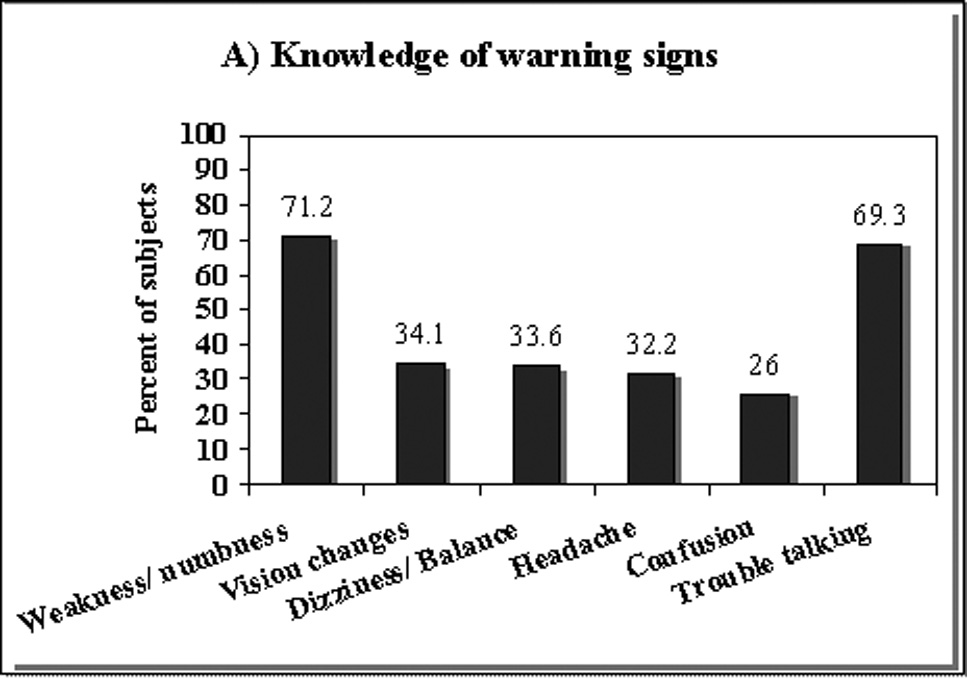
Conclusions: Women were often unable to identify their health condition as a risk factor for stroke. In addition, many women were not undertaking primary prevention behaviors. Risk perception was low, and high-risk women perceived their risk of stroke to be the same as their peers. Educational strategies must advocate for and target high-risk women.
Figures
References
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O'Donnell C, Roger V, Sorlie P, Steinberger J, Thom T, Wilson M, Hong Y. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117(4):e25–e146. - PubMed
-
- Seshadri S, Beiser A, Kelly-Hayes M, Kase CS, Au R, Kannel WB, Wolf PA. The lifetime risk of stroke: estimates from the Framingham Study. Stroke. 2006;37(2):345–350. - PubMed
-
- Williams JE, Chimowitz MI, Cotsonis GA, Lynn MJ, Waddy SP WASID Investigators. Gender differences in outcomes among patients with symptomatic intracranial arterial stenosis. Stroke. 2007;38(7):2055–2062. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
