

Supramaximal dose of candesartan in proteinuric renal disease
- PMID: 19211712
- PMCID: PMC2663827
- DOI: 10.1681/ASN.2008040416
Supramaximal dose of candesartan in proteinuric renal disease
Abstract
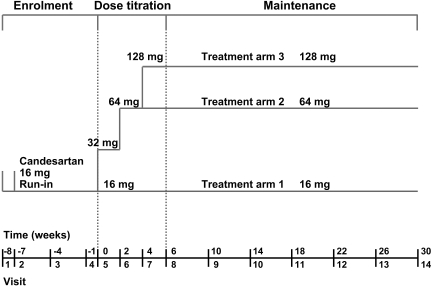
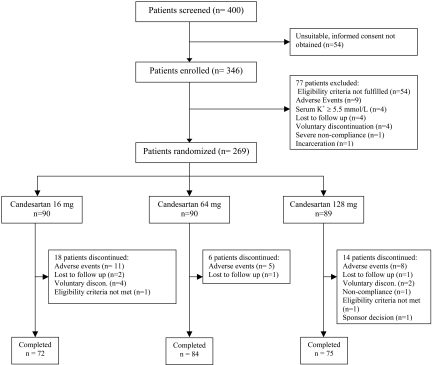
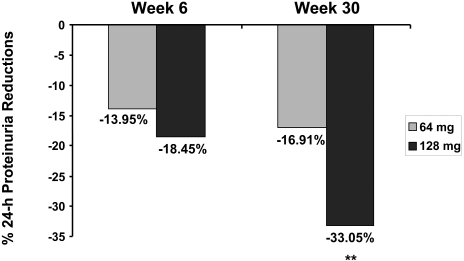
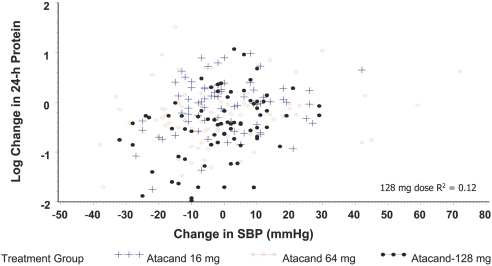
High levels of proteinuria predict renal deterioration, suggesting that interventions to reduce proteinuria may postpone the development of severe renal impairment. This multicenter Canadian trial evaluated whether supramaximal dosages of candesartan would reduce proteinuria to a greater extent than the maximum approved antihypertensive dosage. The authors randomly assigned 269 patients who had persistent proteinuria (> or =1 g/d) despite 7 wk of treatment with the highest approved dosage of candesartan (16 mg/d) to 16, 64, or 128 mg/d candesartan for 30 wk. The median serum creatinine level was 130.0 micromol/L (1.47 mg/dl), and the median urinary protein excretion was 2.66 g/d; most (53.9%) patients had diabetic nephropathy. The mean difference of the percentage change in proteinuria for patients receiving 128 mg/d candesartan compared with those receiving 16 mg/d candesartan was -33.05% (95% confidence interval -45.70 to -17.44; P < 0.0001). Reductions in BP were not different across the three treatment groups. Elevated serum potassium levels (K+ > 5.5 mEq/L) led to the early withdrawal of 11 patients, but there were no dosage-related increases in adverse events. In conclusion, proteinuria that persists despite treatment with the maximum recommended dosage of candesartan can be reduced by increasing the dosage of candesartan further, but serum potassium levels should be monitored during treatment.
Trial registration: ClinicalTrials.gov NCT00242346.
Figures
Comment in
-
Drug dosing for renoprotection: maybe it's time for a drug efficacy-safety score?J Am Soc Nephrol. 2009 Apr;20(4):688-9. doi: 10.1681/ASN.2009020172. Epub 2009 Mar 11. J Am Soc Nephrol. 2009. PMID: 19279124 No abstract available.
References
-
- Brenner BM, Cooper ME, deZeeuw D, Keane WF, Mitch WE, Parving H-H, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S, RENAAL Study Investigators: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 - PubMed
-
- Ruggenenti P, Perna A, Mosconi L, Pisoni R, Remuzzi G: Urinary protein excretion rate is the best independent predictor of ESRF in non-diabetic proteinuric chronic nephropathies. “Gruppo Italiano di Studi Epidemiologici in Nefrologia” (GISEN). Kidney Int 53: 1209–1216, 1998 - PubMed
-
- De Zeeuw D, Remuzzi G, Parving H-H, Keane WF, Zhang Z, Shahinfar S, Snapinn S, Cooper ME, Mitch WE, Brenner BM: Albuminuria, a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathy. Circulation 110: 921–927, 2004 - PubMed
-
- de Zeeuw D, Remuzzi G, Parving H-H, Keane WF, Zhang Z, Shahinfar S, Snapinn S, Cooper ME, Mitch WE, Brenner BM: Proteinuria, a target for renoprotection in patients with type 2 diabetic nephropathy: Lessons from RENAAL. Kidney Int 65: 2309–2320, 2004 - PubMed
-
- Eijkelkamp WBA, Zhang Z, Remuzzi G, Parving H-H, Cooper ME, Keane WF, Shahinfar S, Gleim GW, Weir MR, Brenner BM, de Zeeuw D: Albuminuria is a target for renoprotective therapy independent from blood pressure in patients with type 2 diabetic nephropathy: Post hoc analysis from the Reduction of Endpoints in NIDDM with Angiotensin II Antagonist Losartan (RENAAL) trial. J Am Soc Nephrol 18: 1540–1546, 2007 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
