

Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies
- PMID: 19211817
- PMCID: PMC2676998
- DOI: 10.3945/ajcn.2008.27124
Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies
Abstract
Background: Saturated fatty acid (SFA) intake increases plasma LDL-cholesterol concentrations; therefore, intake should be reduced to prevent coronary heart disease (CHD). Lower habitual intakes of SFAs, however, require substitution of other macronutrients to maintain energy balance.
Objective: We investigated associations between energy intake from monounsaturated fatty acids (MUFAs), polyunsaturated fatty acids (PUFAs), and carbohydrates and risk of CHD while assessing the potential effect-modifying role of sex and age. Using substitution models, our aim was to clarify whether energy from unsaturated fatty acids or carbohydrates should replace energy from SFAs to prevent CHD.
Design: This was a follow-up study in which data from 11 American and European cohort studies were pooled. The outcome measure was incident CHD.
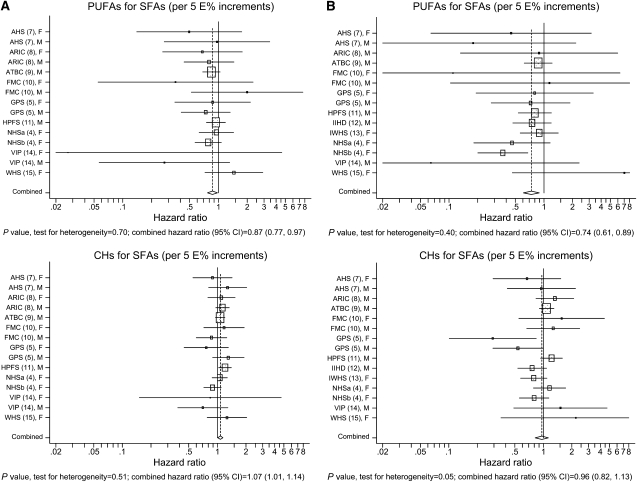
Results: During 4-10 y of follow-up, 5249 coronary events and 2155 coronary deaths occurred among 344,696 persons. For a 5% lower energy intake from SFAs and a concomitant higher energy intake from PUFAs, there was a significant inverse association between PUFAs and risk of coronary events (hazard ratio: 0.87; 95% CI: 0.77, 0.97); the hazard ratio for coronary deaths was 0.74 (95% CI: 0.61, 0.89). For a 5% lower energy intake from SFAs and a concomitant higher energy intake from carbohydrates, there was a modest significant direct association between carbohydrates and coronary events (hazard ratio: 1.07; 95% CI: 1.01, 1.14); the hazard ratio for coronary deaths was 0.96 (95% CI: 0.82, 1.13). MUFA intake was not associated with CHD. No effect modification by sex or age was found.
Conclusion: The associations suggest that replacing SFAs with PUFAs rather than MUFAs or carbohydrates prevents CHD over a wide range of intakes.
Figures
Comment in
-
Omega-6 polyunsaturated fatty acids and coronary heart disease.Am J Clin Nutr. 2009 May;89(5):1283-4. doi: 10.3945/ajcn.2009.27744. Epub 2009 Mar 25. Am J Clin Nutr. 2009. PMID: 19321556 No abstract available.
-
The evidence-based Mediterranean diet reduces coronary heart disease risk, and plant-derived monounsaturated fats may reduce coronary heart disease risk.Am J Clin Nutr. 2009 Sep;90(3):697-8; author reply 698-9. doi: 10.3945/ajcn.2009.28148. Epub 2009 Jul 15. Am J Clin Nutr. 2009. PMID: 19605568 No abstract available.
References
-
- Hu FB, Manson JE, Willett WC. Types of dietary fat and risk of coronary heart disease: a critical review. J Am Coll Nutr 2001;20:5–19 - PubMed
-
- Krauss RM, Eckel RH, Howard B, et al. AHA dietary guidelines: revision 2000: a statement for healthcare professionals from the Nutrition Committee of the American Heart Association. Circulation 2000;102:2284–99 - PubMed
-
- Nordic Nutrition Recommendations 2004 Integrating nutrition and physical activity. Copenhagen, Denmark: Nordic Council of Ministers, 2004
-
- Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med 1997;337:1491–9 - PubMed
-
- Jakobsen MU, Overvad K, Dyerberg J, Schroll M, Heitmann BL. Dietary fat and risk of coronary heart disease: possible effect modification by gender and age. Am J Epidemiol 2004;160:141–9 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
