

Quantitative analysis of intraventricular dyssynchrony using wall thickness by multidetector computed tomography
- PMID: 19212461
- PMCID: PMC2638758
- DOI: 10.1016/j.jcmg.2008.07.014
Quantitative analysis of intraventricular dyssynchrony using wall thickness by multidetector computed tomography
Abstract
Objectives: We sought to determine the feasibility of cardiac computed tomography (CT) to detect significant differences in the extent of left ventricular dyssynchrony in heart failure (HF) patients with wide QRS, HF patients with narrow QRS, and age-matched controls.
Background: The degree of mechanical dyssynchrony has been suggested as a predictor of response to cardiac resynchronization therapy. There have been no published reports of dyssynchrony assessment with the use of CT.
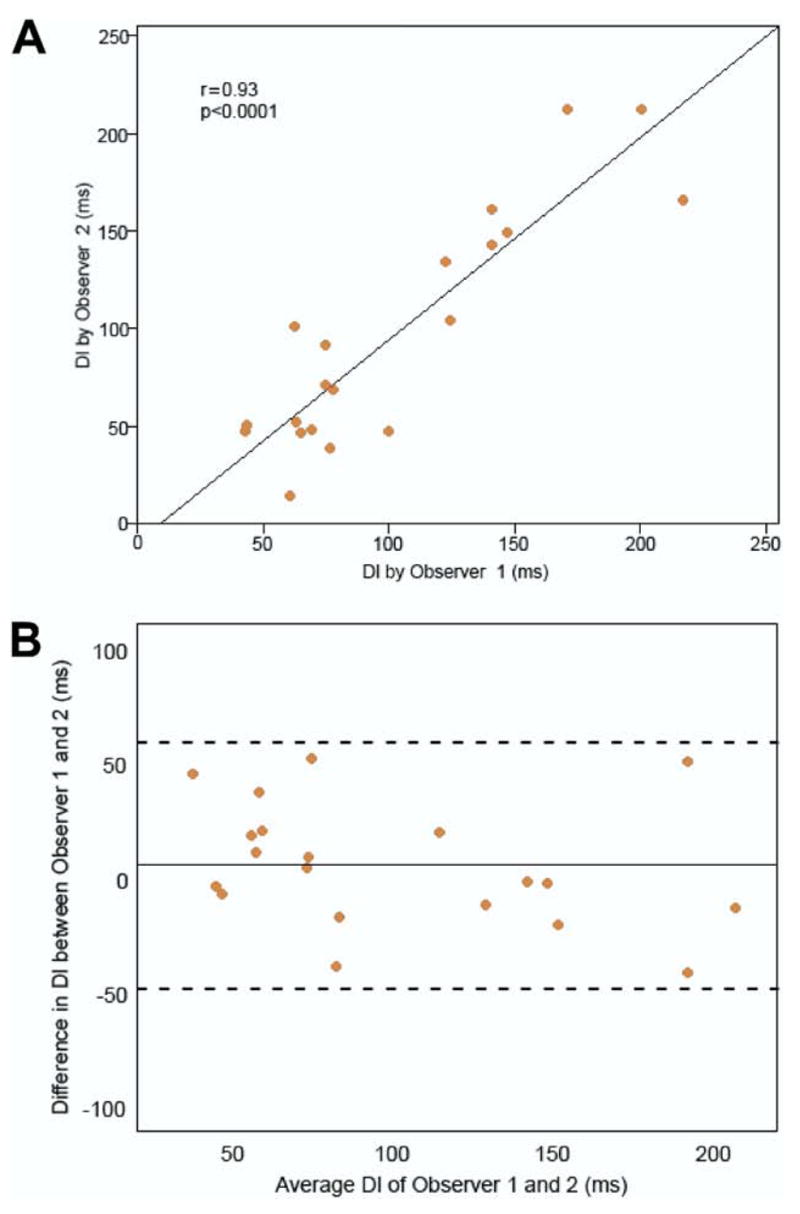
Methods: Thirty-eight subjects underwent electrocardiogram-gated contrast-enhanced 64-slice multidetector CT. The left ventricular endocardial and epicardial boundaries were delineated from short-axis images reconstructed at 10% phase increments of the cardiac cycle. Global and segmental CT dyssynchrony metrics that used changes in wall thickness, wall motion, and volume over time were assessed for reproducibility. We defined a global metric using changes in wall thickness as the dyssynchrony index (DI).
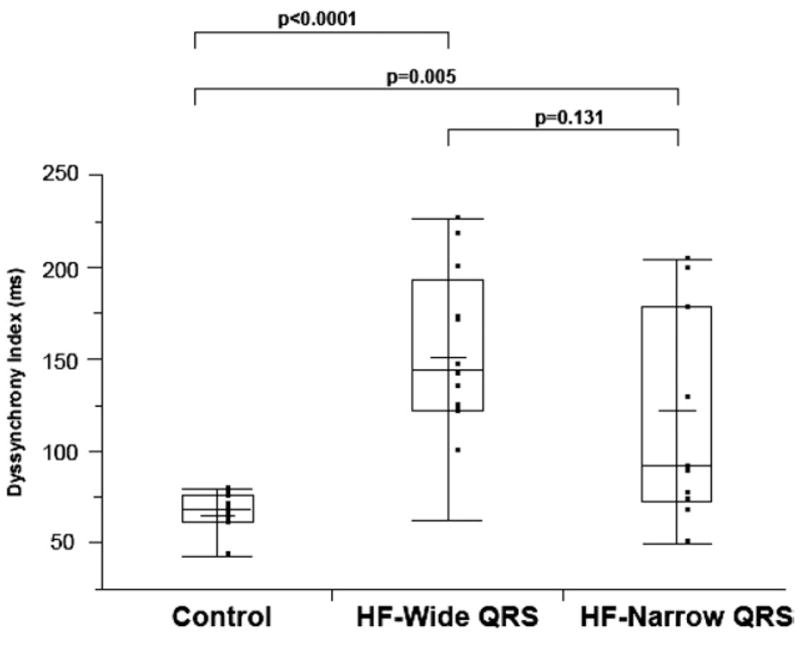
Results: The DI was the most reproducible metric (interobserver and intraobserver intraclass correlation coefficients >/=0.94, p < 0.0001) and was used to determine differences between the 3 groups: HF-wide QRS group (ejection fraction [EF] 22 +/- 8%, QRS 163 +/- 28 ms), HF-narrow QRS (EF 26 +/- 7%, QRS 96 +/- 11 ms), and age-matched control subjects (EF 64 +/- 5%, QRS 87 +/- 9 ms). Mean DI was significantly different between the 3 groups (HF-wide QRS: 152 +/- 44 ms, HF-narrow QRS: 121 +/- 58 ms, and control subjects: 65 +/- 12 ms; p < 0.0001) and greater in the HF-wide QRS (p < 0.0001) and HF-narrow QRS (p = 0.005) groups compared with control subjects. We found that DI had a good correlation with 2-dimensional (r = 0.65, p = 0.012) and 3-dimensional (r = 0.68, p = 0.008) echocardiographic dyssynchrony.
Conclusions: Quantitative assessment of global CT-derived DI, based on changes in wall thickness over time, is highly reproducible and renders significant differences between subjects most likely to have dyssynchrony and age-matched control subjects.
Keywords: dyssynchrony; heart failure; imaging; pacing; tomography.
Figures

References
-
- Gregoratos G, Abrams J, Epstein AE, et al. ACC/AHA/NASPE 2002 guideline update for implantation of cardiac pacemakers and antiarrhythmia devices—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/NASPE Committee to Update the 1998 Pacemaker Guidelines) J Am Coll Cardiol. 2002;40:1703–19. - PubMed
-
- Vardas PE, Auricchio A, Blanc JJ, et al. Guidelines for cardiac pacing and cardiac resynchronization therapy: the task force for cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology. Developed in collaboration with the European Heart Rhythm Association. Eur Heart J. 2007;28:2256–95. - PubMed
-
- Bax JJ, Abraham T, Barold SS, et al. Cardiac resynchronization therapy: part 1—issues before device implantation. J Am Coll Cardiol. 2005;46:2153–67. - PubMed
-
- Bax JJ, Abraham T, Barold SS, et al. Cardiac resynchronization therapy: part 2—issues during and after device implantation and unresolved questions. J Am Coll Cardiol. 2005;46:2168–82. - PubMed
-
- Notabartolo D, Merlino JD, Smith AL, et al. Usefulness of the peak velocity difference by tissue Doppler imaging technique as an effective predictor of response to cardiac resynchronization therapy. Am J Cardiol. 2004;94:817–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
