

Minimum 2-year outcome of cervical laminoplasty with deep extensor muscle-preserving approach: impact on cervical spine function and quality of life
- PMID: 19214599
- PMCID: PMC3234000
- DOI: 10.1007/s00586-009-0892-1
Minimum 2-year outcome of cervical laminoplasty with deep extensor muscle-preserving approach: impact on cervical spine function and quality of life
Abstract
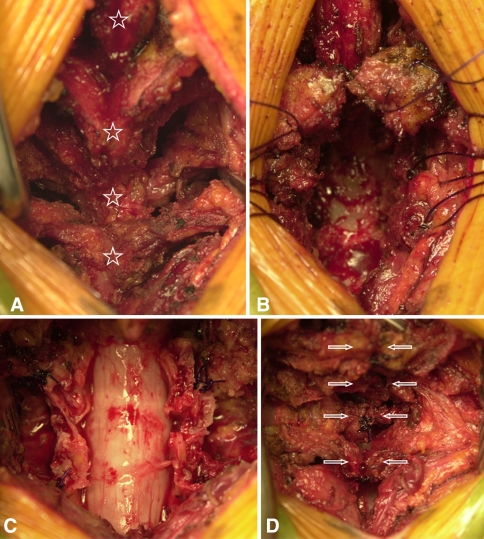
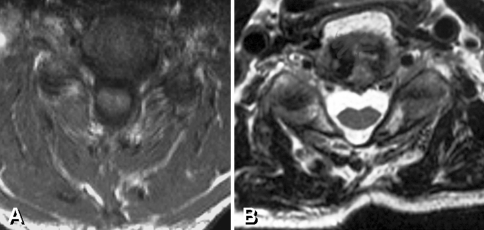
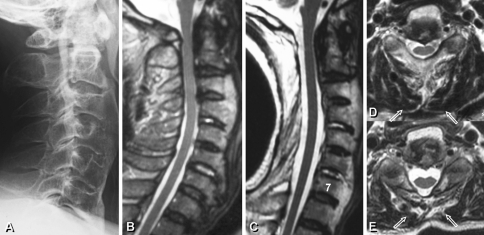
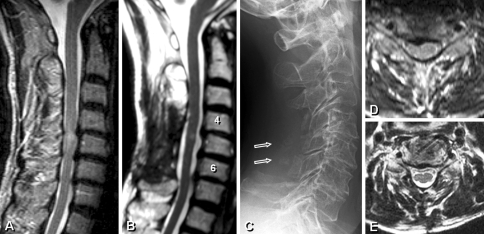
In this retrospective cohort study, two surgical methods of conventional open-door laminoplasty and deep extensor muscle-preserving laminoplasty were allocated for the treatment of cervical myelopathy, and were specifically compared in terms of axial pain, cervical spine function, and quality of life (QOL) with a minimum follow-up period of 2 years. Eighty-four patients were divided into two groups and received either a conventional open-door laminoplasty (CL group) or laminoplasty using a deep extensor muscle-preserving approach (MP group). The latter approach was performed by preserving multifidus and semispinalis cervicis attachments followed by open-door laminoplasty and re-suture of the bisected spinous processes at each decompression level. The average follow-up period was 38 months (25-53 months). The preoperative and follow-up evaluations included the original Japanese Orthopaedic Association (JOA) score, the new tentative JOA score including cervical spine function and QOL, and the visual analogue scale (VAS) of axial pain. Radiological analyses included cervical lordosis and flexion-extension range of motion (flex-ext ROM) (C2-7), and deep extensor muscle areas on MR axial images. The JOA recovery rates were statistically equivalent between two groups. The MP group demonstrated a statistically superior cervical spine function (84% vs 63%) and QOL (61% vs 45%) when compared to the CL group at final follow-up (P < 0.05). The average VAS scores at final follow-up were 2.3 and 4.9 in MP and CL groups (P < 0.05). The cervical lordosis and flex-ext ROM were statistically equivalent. The percent deep muscle area on MRI demonstrated a significant atrophy in CL group compared to that in MP group (56% vs 88%; P < 0.01). Laminoplasty employing the deep extensor muscle-preserving approach appeared to be effective in reducing the axial pain and deep muscle atrophy as well as improving cervical spine function and QOL when compared to conventional open-door laminoplasty.
Figures
References
-
- Hirabayashi K, Toyama Y. Choice of surgical procedure for cervical ossification of the posterior longitudinal ligaments. In: Yonenobu K, Sakou T, Ono K, editors. ossification of the posterior longitudinal ligament. Tokyo: Springer; 1997. pp. 135–142.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
