

Review
doi: 10.1016/j.emc.2008.09.002.
Vertigo and dizziness in the emergency department
Affiliations
- PMID: 19218018
- PMCID: PMC2676794
- DOI: 10.1016/j.emc.2008.09.002
Item in Clipboard
Review
Vertigo and dizziness in the emergency department
Emerg Med Clin North Am.
2009 Feb.
Abstract
Understanding three peripheral vestibular disorders--vestibular neuritis, benign paroxysmal positional vertigo, and Meniere's disease--is the key to the evaluation and management of vertigo and dizziness presentations in the emergency department. Each of these benign disorders is a common cause of a broad category of dizziness presentation. In addition, each of these disorders has characteristic features that allow for a bedside diagnosis. An effective strategy for "ruling-out" a serious disorder, such as stroke, is "ruling-in" a peripheral vestibular disorder. In this article a focus is on the key features of these disorders.
Figures
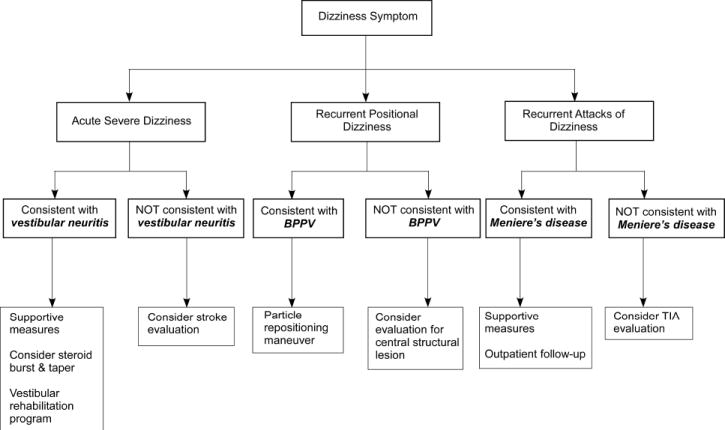
Diagnostic and management algorithm for common dizziness presentation categories. BPPV = benign paroxysmal positional vertigo; TIA = transient ischemic attack.
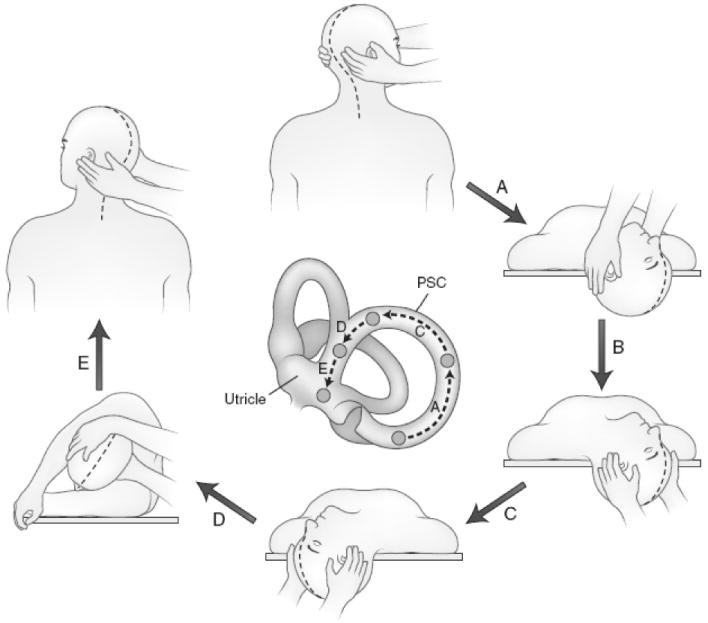
Epley maneuver for treatment of posterior canal benign paroxysmal positional vertigo affecting the right ear. The procedure can be reversed for treating the left ear. The drawing of the labyrinth in the center shows the position of the debris as it moves around the posterior semicircular canal (PSC) and into the utricle (UT). The patient is seated upright, with head facing the examiner, who is standing on the right. (A) The patient is then rapidly moved to head-hanging right position (Dix-Hallpike test). This position is maintained until the nystagmus ceases. (B) The examiner moves to the head of the table, repositioning hands as shown. (C) The head is rotated quickly to the left with right ear upward. This position is maintained for 30 seconds. (D) The patient rolls onto the left side while the examiner rapidly rotates the head leftward until the nose is directed toward the floor. This position is then held for 30 seconds. (E) The patient is rapidly lifted into the sitting position, now facing left. The entire sequence should be repeated until no nystagmus can be elicited. Following the maneuver, the patient is instructed to avoid head hanging positions to prevent the debris from reentering the posterior canal. From: Rakel RE. Conn’s Current Therapy 1995, p.839, WB Saunders, 1995. Permission granted by Elsevier Ltd.
References
-
- Burt CW, Schappert SM. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 1999--2000. Vital Health Stat. 2004 Sep 13;(157):1–70. - PubMed
-
- Newman-Toker DE, Cannon LM, Stofferahn ME, Rothman RE, Hsieh YH, Zee DS. Imprecision in patient reports of dizziness symptom quality: a cross-sectional study conducted in an acute care setting. Mayo Clin Proc. 2007 Nov;82(11):1329–1340. - PubMed
-
- Norrving B, Magnusson M, Holtas S. Isolated acute vertigo in the elderly; vestibular or vascular disease? Acta Neurol Scand. 1995 Jan;91(1):43–48. - PubMed
-
- Lee H, Cho YW. A case of isolated nodulus infarction presenting as a vestibular neuritis. J Neurol Sci. 2004 Jun 15;221(12):117–119. - PubMed
-
- Lee H, Sohn SI, Cho YW, et al. Cerebellar infarction presenting isolated vertigo: frequency and vascular topographical patterns. Neurology. 2006 Oct 10;67(7):1178–1183. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
