

Modification of the effect of vitamin E supplementation on the mortality of male smokers by age and dietary vitamin C
- PMID: 19218294
- PMCID: PMC2661323
- DOI: 10.1093/aje/kwn413
Modification of the effect of vitamin E supplementation on the mortality of male smokers by age and dietary vitamin C
Abstract
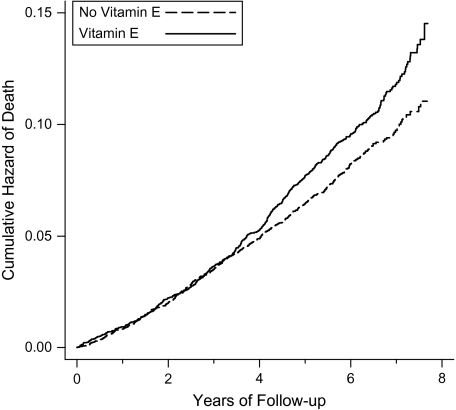
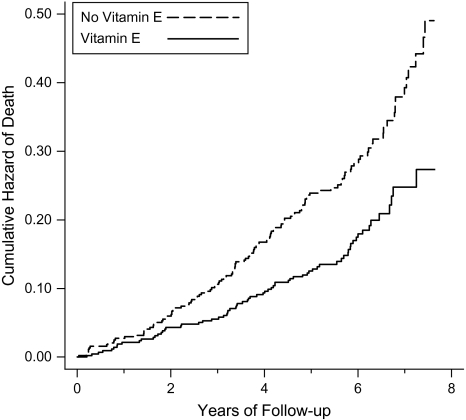
The Alpha-Tocopherol, Beta-Carotene Cancer Prevention (ATBC) Study (1985-1993) recruited 29,133 Finnish male cigarette smokers, finding that vitamin E supplementation had no overall effect on mortality. The authors of this paper found that the effect of vitamin E on respiratory infections in ATBC Study participants was modified by age, smoking, and dietary vitamin C intake; therefore, they examined whether the effect of vitamin E supplementation on mortality is modified by the same variables. During a median follow-up time of 6.1 years, 3,571 deaths occurred. Age and dietary vitamin C intake had a second-order interaction with vitamin E supplementation of 50 mg/day. Among participants with a dietary vitamin C intake above the median of 90 mg/day, vitamin E increased mortality among those aged 50-62 years by 19% (95% confidence interval: 5, 35), whereas vitamin E decreased mortality among those aged 66-69 years by 41% (95% CI: -56, -21). Vitamin E had no effect on participants who had a dietary vitamin C intake below the median. Smoking quantity did not modify the effect of vitamin E. This study provides strong evidence that the effect of vitamin E supplementation on mortality varies between different population groups. Further study is needed to confirm this heterogeneity.
Figures
References
-
- Radimer K, Bindewald B, Hughes J, et al. Dietary supplement use by US adults: data from the National Health and Nutrition Examination Survey, 1999–2000. Am J Epidemiol. 2004;160(4):339–349. - PubMed
-
- Beckman KB, Ames BN. The free radical theory of aging matures. Physiol Rev. 1998;78(2):547–581. - PubMed
-
- Finkel T, Holbrook NJ. Oxidants, oxidative stress and the biology of ageing. Nature. 2000;408(6809):239–247. - PubMed
-
- Vivekananthan DP, Penn MS, Sapp SK, et al. Use of antioxidant vitamins for the prevention of cardiovascular disease: meta-analysis of randomised trials. Lancet. 2003;361(9374):2017–2023. - PubMed
-
- Miller ER, Pastor-Barriuso R, Dalal D, et al. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med. 2005;142(1):37–46. (Comments: Ann Intern Med. 2005;143(2):150–158) - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
