

Fabry disease: progression of nephropathy, and prevalence of cardiac and cerebrovascular events before enzyme replacement therapy
- PMID: 19218538
- PMCID: PMC2698092
- DOI: 10.1093/ndt/gfp031
Fabry disease: progression of nephropathy, and prevalence of cardiac and cerebrovascular events before enzyme replacement therapy
Abstract
Background: In Fabry disease, progressive glycolipid accumulation leads to organ damage and early demise, but the incidence of renal, cardiac and cerebrovascular events has not been well characterized.
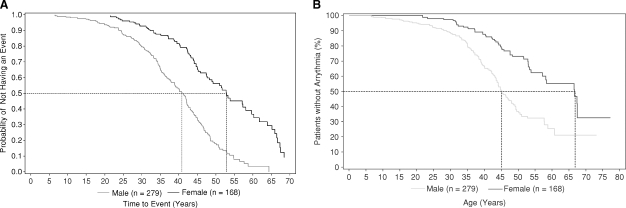
Methods: We conducted a retrospective chart review of 279 affected males and 168 females from 27 sites (USA, Canada, Europe). The pre-defined study endpoints included progression of renal, cardiac and cerebrovascular involvement and/or death before the initiation of enzyme replacement therapy.
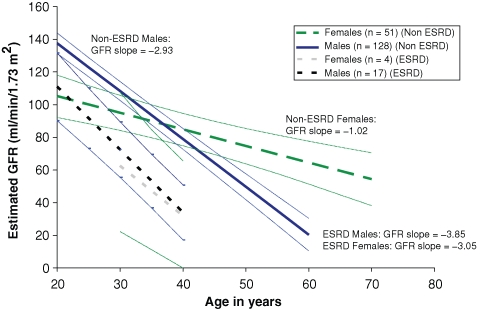
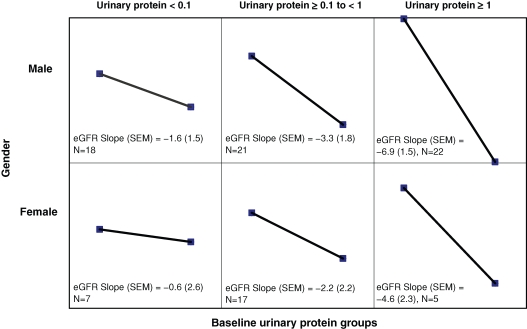
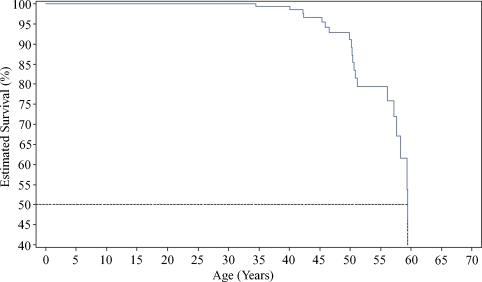
Results: The mean rate of estimated glomerular filtration rate (eGFR) decline for patients was -2.93 for males, and -1.02 ml/min/1.73 m(2)/year for females. Prevalence and severity of proteinuria, baseline eGFR <60 ml/min/1.73 m(2) and hypertension were associated with more rapid loss of eGFR. Advanced Fabry nephropathy was more prevalent and occurred earlier among males than females. Cardiac events (mainly arrhythmias), strokes and transient ischaemic attacks occurred in 49, 11, 6% of males, and in 35, 8, 4% of females, respectively. The mean age at death for 20 male patients was 49.9 years.
Conclusions: Baseline proteinuria, reduced baseline eGFR, hypertension and male gender were associated with more rapid progression of Fabry nephropathy. The eGFR progression rate may increase with advancing nephropathy, and may differ between subgroups of patients with Fabry disease.
Figures
References
-
- Desnick R, Ioannou Y, Eng C. Alpha-galactosidase a deficiency: fabry disease. In: Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The Metabolic and Molecular Bases of Inherited Disease. 8th edn. New York: McGraw-Hill; 2001. pp. 3733–3774.
-
- Gubler MC, Lenoir G, Grunfeld JP, et al. Early renal changes in hemizygous and heterozygous patients with Fabry's disease. Kidney Int. 1978;13:223–235. - PubMed
-
- Sessa A, Meroni M, Battini G, et al. Renal pathological changes in Fabry disease. J Inherit Metab Dis. 2001;24:66–70. - PubMed
-
- Thurberg BL, Rennke H, Colvin RB, et al. Globotriaosylceramide accumulation in the Fabry kidney is cleared from multiple cell types after enzyme replacement therapy. Kidney Int. 2002;62:1933–1946. - PubMed
-
- Tøndel C, Bostad L, Hirth A, et al. Renal biopsy findings in children and adolescents with Fabry disease and minimal albuminuria. Am J Kidney Dis. 2008;51:767–776. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
