

Treatment of war wounds: a historical review
- PMID: 19219516
- PMCID: PMC2706344
- DOI: 10.1007/s11999-009-0738-5
Treatment of war wounds: a historical review
Abstract
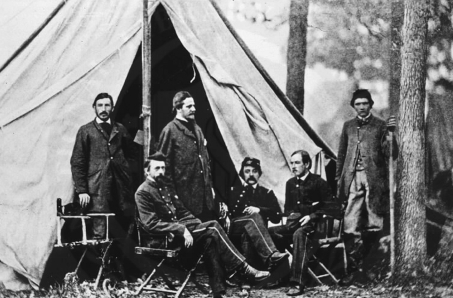
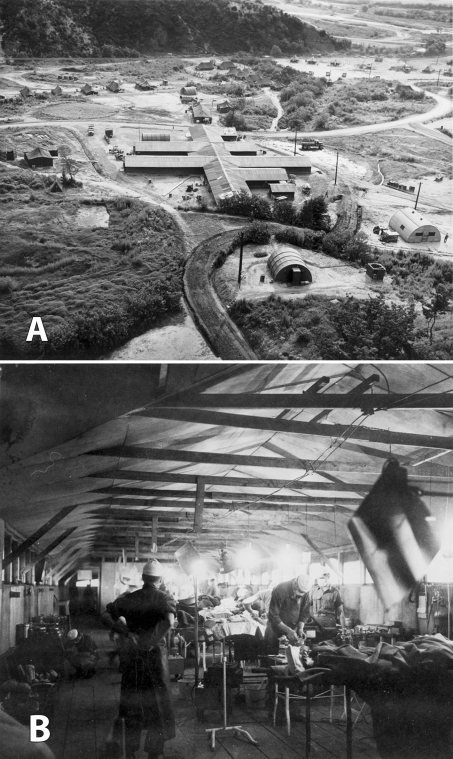
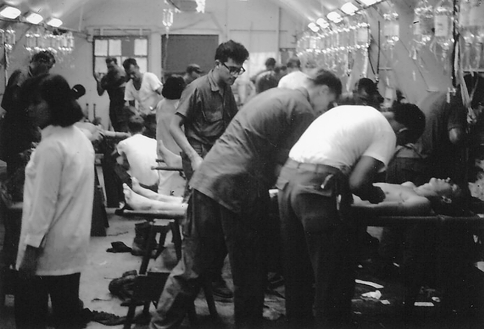
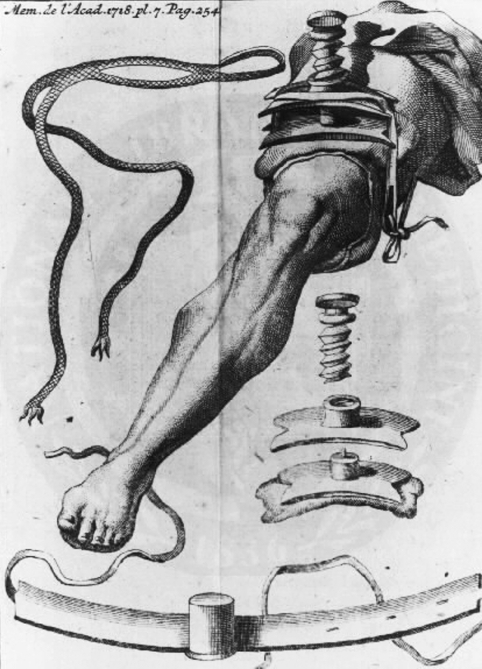
The treatment of war wounds is an ancient art, constantly refined to reflect improvements in weapons technology, transportation, antiseptic practices, and surgical techniques. Throughout most of the history of warfare, more soldiers died from disease than combat wounds, and misconceptions regarding the best timing and mode of treatment for injuries often resulted in more harm than good. Since the 19th century, mortality from war wounds steadily decreased as surgeons on all sides of conflicts developed systems for rapidly moving the wounded from the battlefield to frontline hospitals where surgical care is delivered. We review the most important trends in US and Western military trauma management over two centuries, including the shift from primary to delayed closure in wound management, refinement of amputation techniques, advances in evacuation philosophy and technology, the development of antiseptic practices, and the use of antibiotics. We also discuss how the lessons of history are reflected in contemporary US practices in Iraq and Afghanistan.
Figures






References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '6388417', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/6388417/'}]}
- Aldrete JA, Marron GM, Wright AJ. The first administration of anesthesia in military surgery: on occasion of the Mexican-American War. Anesthesiology. 1984;61:585–588. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '10511234', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10511234/'}]}
- American Society of Health-System Pharmacists. Armed Services Blood Program therapeutic guidelines on antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 1999;56:1839–1888. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '17003202', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17003202/'}]}
- Andersen RC, Frisch HM, Farber GL, Hayda RA. Definitive treatment of combat casualties at military medical centers. J Am Acad Orthop Surg. 2006;14:S24–S31. - PubMed
-
- None
- Anderson R. An automatic method for treatment of fractures of the tibia and the fibula. J Bone Joint Surg Am. 1934;58:639–646.
-
- Artz CP, Bronwell AW, Sako Y. Preoperative and postoperative care of battle casualties. Available at: http://history.amedd.army.mil/booksdocs/korea/recad1/frameindex.html. Accessed Sept. 12, 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
