

Fluid mechanics of artificial heart valves
- PMID: 19220329
- PMCID: PMC2752693
- DOI: 10.1111/j.1440-1681.2008.05099.x
Fluid mechanics of artificial heart valves
Abstract
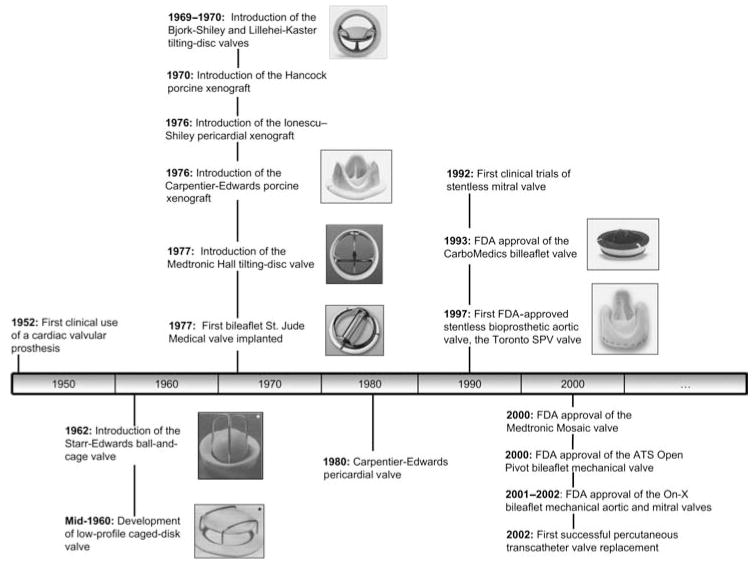
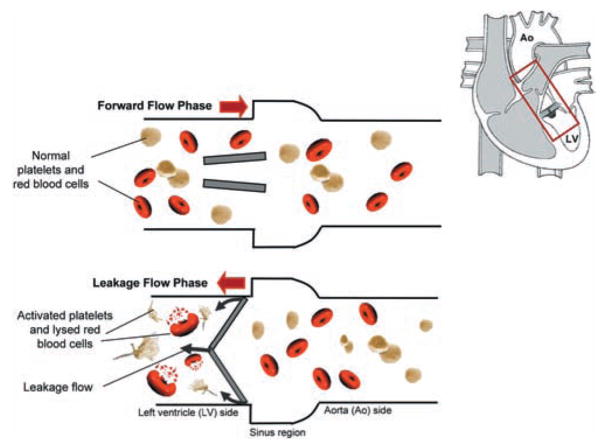
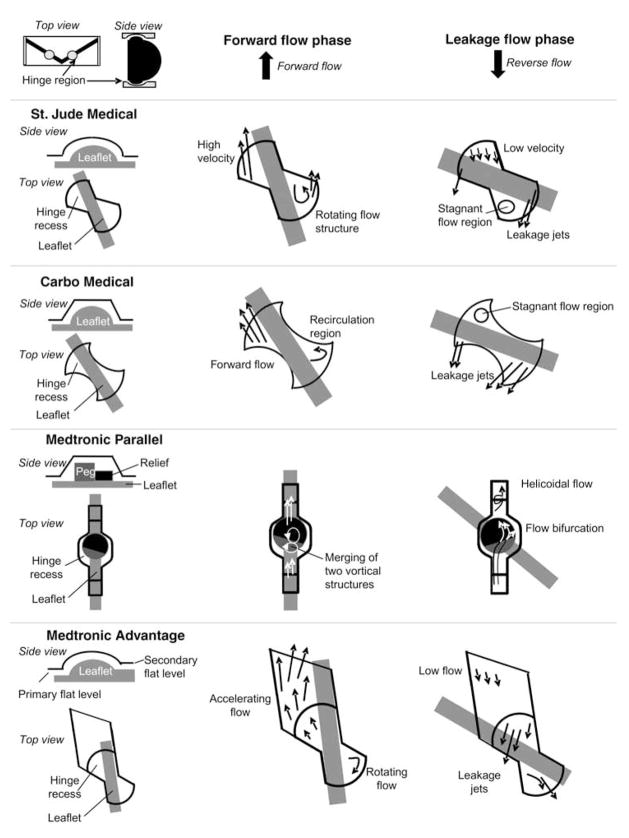
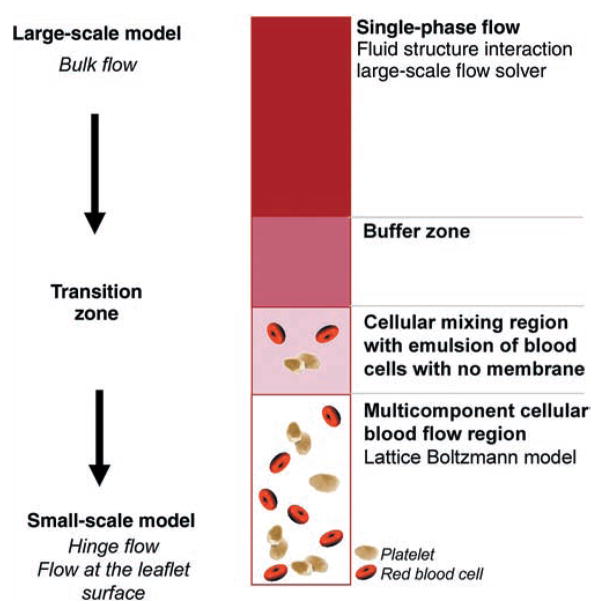
1. Artificial heart valves have been in use for over five decades to replace diseased heart valves. Since the first heart valve replacement performed with a caged-ball valve, more than 50 valve designs have been developed, differing principally in valve geometry, number of leaflets and material. To date, all artificial heart valves are plagued with complications associated with haemolysis, coagulation for mechanical heart valves and leaflet tearing for tissue-based valve prosthesis. For mechanical heart valves, these complications are believed to be associated with non-physiological blood flow patterns. 2. In the present review, we provide a bird's-eye view of fluid mechanics for the major artificial heart valve types and highlight how the engineering approach has shaped this rapidly diversifying area of research. 3. Mechanical heart valve designs have evolved significantly, with the most recent designs providing relatively superior haemodynamics with very low aerodynamic resistance. However, high shearing of blood cells and platelets still pose significant design challenges and patients must undergo life-long anticoagulation therapy. Bioprosthetic or tissue valves do not require anticoagulants due to their distinct similarity to the native valve geometry and haemodynamics, but many of these valves fail structurally within the first 10-15 years of implantation. 4. These shortcomings have directed present and future research in three main directions in attempts to design superior artificial valves: (i) engineering living tissue heart valves; (ii) development of advanced computational tools; and (iii) blood experiments to establish the link between flow and blood damage.
Figures

Similar articles
-
Fluid mechanics of heart valves.Annu Rev Biomed Eng. 2004;6:331-62. doi: 10.1146/annurev.bioeng.6.040803.140111. Annu Rev Biomed Eng. 2004. PMID: 15255773 Review.
-
Aortic Valve Replacement.2023 May 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 May 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30725821 Free Books & Documents.
-
Mechanical considerations for polymeric heart valve development: Biomechanics, materials, design and manufacturing.Biomaterials. 2019 Dec;225:119493. doi: 10.1016/j.biomaterials.2019.119493. Epub 2019 Sep 17. Biomaterials. 2019. PMID: 31569017 Free PMC article. Review.
-
Effects of valve geometry and tissue anisotropy on the radial stretch and coaptation area of tissue-engineered heart valves.J Biomech. 2013 Jul 26;46(11):1792-800. doi: 10.1016/j.jbiomech.2013.05.015. Epub 2013 Jun 18. J Biomech. 2013. PMID: 23786664
-
Impact of Clinically Relevant Elliptical Deformations on the Damage Patterns of Sagging and Stretched Leaflets in a Bioprosthetic Heart Valve.Cardiovasc Eng Technol. 2018 Sep;9(3):351-364. doi: 10.1007/s13239-018-0366-x. Epub 2018 Jun 12. Cardiovasc Eng Technol. 2018. PMID: 29948838 Free PMC article.
Cited by
-
Enhanced discrete phase model for multiphase flow simulation of blood flow with high shear stress.Sci Prog. 2021 Jan-Mar;104(1):368504211008064. doi: 10.1177/00368504211008064. Sci Prog. 2021. PMID: 33788651 Free PMC article.
-
Percutaneous Double Lumen Cannula for Right Ventricle Assist Device System: A Computational Fluid Dynamics Study.Biocybern Biomed Eng. 2016;36(3):482-490. doi: 10.1016/j.bbe.2016.04.002. Epub 2016 Apr 18. Biocybern Biomed Eng. 2016. PMID: 27570334 Free PMC article.
-
Development of Tissue Engineered Heart Valves for Percutaneous Transcatheter Delivery in a Fetal Ovine Model.JACC Basic Transl Sci. 2020 Jul 29;5(8):815-828. doi: 10.1016/j.jacbts.2020.06.009. eCollection 2020 Aug. JACC Basic Transl Sci. 2020. PMID: 32875171 Free PMC article.
-
Assessment Parameters for Arrayed Pulse Wave Analysis and Application in Hypertensive Disorders.Evid Based Complement Alternat Med. 2022 Feb 17;2022:6652028. doi: 10.1155/2022/6652028. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 35222674 Free PMC article.
-
Use of sucrose to diminish pore formation in freeze-dried heart valves.Sci Rep. 2018 Aug 28;8(1):12982. doi: 10.1038/s41598-018-31388-4. Sci Rep. 2018. PMID: 30154529 Free PMC article.
References
-
- Silverthorn DU. Human Physiology: An Integrated Approach. 4. Benjamin Cummings; San Francisco: 2006.
-
- Yacoub N, Takkenberg J. Will heart valve tissue engineering change the world? Nat Clin Prac Cardiovas Med. 2005;2:60–1. - PubMed
-
- Black MM, Drury N. Mechanical and other problems in artificial valves. In: Berry C, editor. Pathology of Devices, Vol. 84, Current Topics in Pathology. Springer-Verlag; Heidelberg: 1994. pp. 127–59. - PubMed
-
- Wurzinger LJ, Opitz R, Wolf M, Schmidschonbein H. Shear induced platelet activation: A critical reappraisal. Biorheology. 1985;22:399–413. - PubMed
-
- Ramstack JM, Zuckerman L, Mockros LF. Shear-induced activation of platelets. J Biomech. 1979;12:113–25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
