

Combination antiretroviral therapy in population affected by conflict: outcomes from large cohort in northern Uganda
- PMID: 19223338
- PMCID: PMC2645846
- DOI: 10.1136/bmj.b201
Combination antiretroviral therapy in population affected by conflict: outcomes from large cohort in northern Uganda
Abstract
Objective: To measure the clinical and immunological outcomes of HIV positive adult patients receiving combination antiretroviral therapy in conflict affected northern Uganda.
Design: Prospective cohort study.
Setting: Gulu District, northern Uganda.
Participants: 1625 adults (aged over 14 years) receiving combination antiretroviral therapy.
Primary outcome: all cause mortality.
Secondary outcomes: impact of covariates (sex, age, CD4 count at start, adherence, tuberculosis at start, duration of treatment, and internally displaced person status) on mortality.
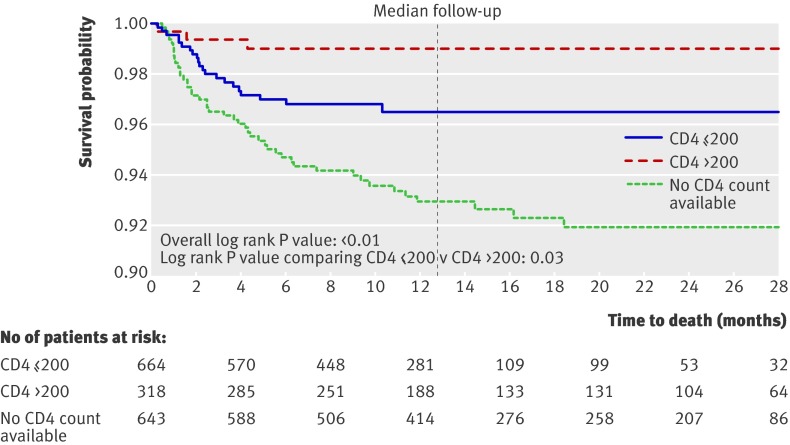
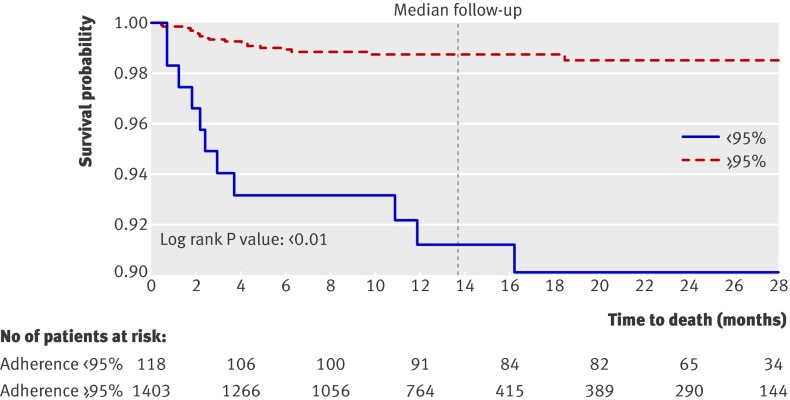
Results: Sixty nine (4.2%) patients died during follow-up. The mortality incidence rate was 3.48 (95% confidence interval 2.66 to 4.31) per 100 person years. Patients started treatment with a median CD4 count of 157 (interquartile range 90-220) cells/mul; most (1009; 63%) had World Health Organization stage 2 defined illness. Sixty two patients had pulmonary tuberculosis at the start of treatment. Of the 1521 patients with adherence data, 118 (7.8%) had adherence of less than 95% and 1403 (92.2%) had adherence of 95% or above.
Conclusion: Patients receiving combination antiretroviral therapy in conflict affected northern Uganda had a mortality comparable to that of patients in peaceful, low income settings and better adherence than patients in higher income settings. These favourable findings highlight the need to expand access to combination antiretroviral therapy in populations affected by armed conflict.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Adherence to combination antiretroviral therapy in complex emergency settings.BMJ. 2009 Feb 18;338:a2662. doi: 10.1136/bmj.a2662. BMJ. 2009. PMID: 19224964 No abstract available.
Similar articles
-
Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda.Ann Intern Med. 2011 Aug 16;155(4):209-16. doi: 10.7326/0003-4819-155-4-201108160-00358. Epub 2011 Jul 18. Ann Intern Med. 2011. PMID: 21768555
-
Clinical and immunological outcomes of a national paediatric cohort receiving combination antiretroviral therapy in Uganda.AIDS. 2008 Nov 30;22(18):2493-9. doi: 10.1097/QAD.0b013e328318f148. AIDS. 2008. PMID: 19005272
-
Good adherence to HAART and improved survival in a community HIV/AIDS treatment and care programme: the experience of The AIDS Support Organization (TASO), Kampala, Uganda.BMC Health Serv Res. 2008 Nov 20;8:241. doi: 10.1186/1472-6963-8-241. BMC Health Serv Res. 2008. PMID: 19021908 Free PMC article.
-
Treatment interruptions predict resistance in HIV-positive individuals purchasing fixed-dose combination antiretroviral therapy in Kampala, Uganda.AIDS. 2007 May 11;21(8):965-71. doi: 10.1097/QAD.0b013e32802e6bfa. AIDS. 2007. PMID: 17457090 Clinical Trial.
-
HIV-1 disease progression and mortality before the introduction of highly active antiretroviral therapy in rural Uganda.AIDS. 2007 Nov;21 Suppl 6:S21-9. doi: 10.1097/01.aids.0000299407.52399.05. AIDS. 2007. PMID: 18032935 Clinical Trial.
Cited by
-
Male gender predicts mortality in a large cohort of patients receiving antiretroviral therapy in Uganda.J Int AIDS Soc. 2011 Nov 3;14:52. doi: 10.1186/1758-2652-14-52. J Int AIDS Soc. 2011. PMID: 22050673 Free PMC article.
-
Impact of tuberculosis on mortality among HIV-infected patients receiving antiretroviral therapy in Uganda: a prospective cohort analysis.AIDS Res Ther. 2013 Jul 13;10(1):19. doi: 10.1186/1742-6405-10-19. AIDS Res Ther. 2013. PMID: 23849301 Free PMC article.
-
Scale-up of HIV treatment through PEPFAR: a historic public health achievement.J Acquir Immune Defic Syndr. 2012 Aug 15;60 Suppl 3(Suppl 3):S96-104. doi: 10.1097/QAI.0b013e31825eb27b. J Acquir Immune Defic Syndr. 2012. PMID: 22797746 Free PMC article. Review.
-
Density of healthcare providers and patient outcomes: evidence from a nationally representative multi-site HIV treatment program in Uganda.PLoS One. 2011 Jan 17;6(1):e16279. doi: 10.1371/journal.pone.0016279. PLoS One. 2011. PMID: 21264224 Free PMC article.
-
Surgery of the femur in HIV positive patients: a retrospective review from 2005 to 2011.Ir J Med Sci. 2015 Jun;184(2):505-10. doi: 10.1007/s11845-014-1156-6. Epub 2014 Jun 11. Ir J Med Sci. 2015. PMID: 24917418
References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. Geneva: WHO, 2007. (available at www.who.int/hiv/mediacentre/univeral_access_progress_report_en.pdf).
-
- Uppsala Conflict Data Program (UCDP). Customized report: active conflicts in Africa. 2006. www.pcr.uu.se/database/CustomizedReport/subset.php.
-
- Steering Committee for Humanitarian Response. The Sphere project: humanitarian charter and minimum standards in disaster response. Geneva: Sphere Project, 2004. (available at www.humanitarianinfo.org/IMToolbox/10_Reference/Sphere_Guidlines_2004/20...). - PubMed
-
- Inter-Agency Standing Committee (IASC). Guidelines for HIV/AIDS interventions in emergency settings. 2003. http://data.unaids.org/Publications/External-Documents/IASC_Guidelines-E....
-
- Spiegel PB. HIV/AIDS among conflict-affected and displaced populations: dispelling myths and taking action. Disasters 2004;28:322-39. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials