

Prospectively validated dosing nomograms for maximizing the pharmacodynamics of vancomycin administered by continuous infusion in critically ill patients
- PMID: 19223642
- PMCID: PMC2681515
- DOI: 10.1128/AAC.01149-08
Prospectively validated dosing nomograms for maximizing the pharmacodynamics of vancomycin administered by continuous infusion in critically ill patients
Abstract
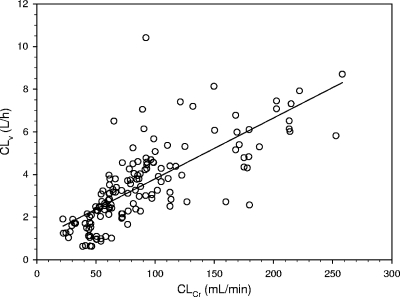
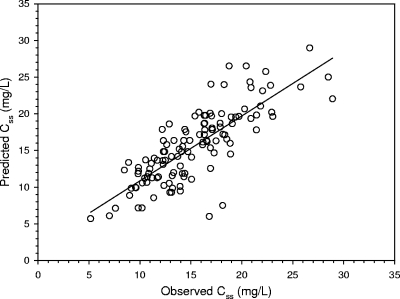
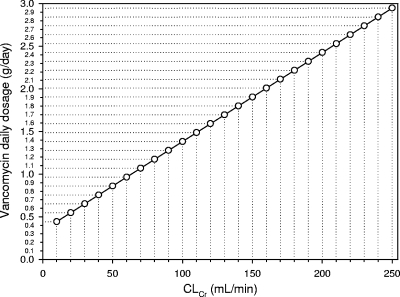
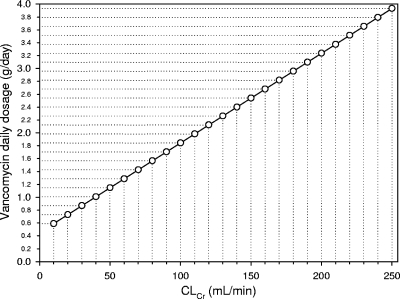
The efficacy of vancomycin against methicillin-resistant Staphylococcus aureus (MRSA)-related infections has been called into question by recent findings of higher rates of failure of vancomycin treatment of infections caused by strains with high MICs. Continuous infusion may be the best way to maximize the time-dependent activity of vancomycin. The aim of this study was to create dosing nomograms in relation to different creatinine clearance (CL(Cr)) estimates for use in daily clinical practice to target the steady-state concentrations (C(ss)s) of vancomycin during continuous infusion at 15 to 20 mg/liter (after the administration of an initial loading dose of 15 mg/kg of body weight over 2 h). The correlation between vancomycin clearance (CL(v)) and CL(Cr) was retrospectively assessed in a cohort of critically ill patients (group 1, n = 70) to create a formula for dosage calculation to target C(ss) at 15 mg/liter. The performance of this formula was prospectively validated in a similar cohort (group 2, n = 63) by comparison of the observed and the predicted C(ss)s. A significant relationship between CL(v) and CL(Cr) was observed in group 1 (P < 0.001). The application of the calculated formula to vancomycin dosing in group 2 {infusion rate (g/24 h) = [0.029 x CL(Cr) (ml/min) + 0.94] x target C(ss) x (24/1,000)} led to a significant correlation between the observed and the predicted C(ss)s (r = 0.80, P < 0.001). Two dosing nomograms based on CL(Cr) were created to target the vancomycin C(ss) at 15 and 20 mg/liter in critically ill patients. These nomograms could be helpful in improving the vancomycin treatment of MRSA infections, especially in the presence of borderline-susceptible pathogens and/or of pathophysiological conditions which may enhance the clearance of vancomycin, while potentially avoiding the increased risk of nephrotoxicity observed with the use of high intermittent doses of vancomycin.
Figures
References
-
- Alos, J. I., A. Garcia-Canas, P. Garcia-Hierro, and F. Rodriguez-Salvanes. 2008. Vancomycin MICs did not creep in Staphylococcus aureus isolates from 2002 to 2006 in a setting with low vancomycin usage. J. Antimicrob. Chemother. 62:773-775. - PubMed
-
- American Thoracic Society and Infectious Diseases Society of America. 2005. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 171:388-416. - PubMed
-
- Cockcroft, D. W., and M. H. Gault. 1976. Prediction of creatinine clearance from serum creatinine. Nephron 16:31-41. - PubMed
-
- Dellinger, R. P., M. M. Levy, J. M. Carlet, J. Bion, M. M. Parker, R. Jaeschke, K. Reinhart, D. C. Angus, C. Brun-Buisson, R. Beale, T. Calandra, J. F. Dhainaut, H. Gerlach, M. Harvey, J. J. Marini, J. Marshall, M. Ranieri, G. Ramsay, J. Sevransky, B. T. Thompson, S. Townsend, J. S. Vender, J. L. Zimmerman, and J. L. Vincent. 2008. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 34:17-60. - PMC - PubMed
-
- Deresinski, S. 2007. Counterpoint: vancomycin and Staphylococcus aureus—an antibiotic enters obsolescence. Clin. Infect. Dis. 44:1543-1548. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
