

The combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over time
- PMID: 19223785
- PMCID: PMC3606956
- DOI: 10.1097/QAI.0b013e31819675e9
The combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over time
Abstract
Objective: To characterize the impact of longitudinal adherence on survival in drug-naive individuals starting currently recommended highly active antiretroviral therapy (HAART) regimens.
Methods: Eligible study participants initiated HAART between January 2000 and November 2004 and were followed until November 2005 (N = 903). HAART regimens contained efavirenz, nevirapine, or ritonavir-boosted atazanavir or lopinavir. Marginal structural modeling was used to address our objective.
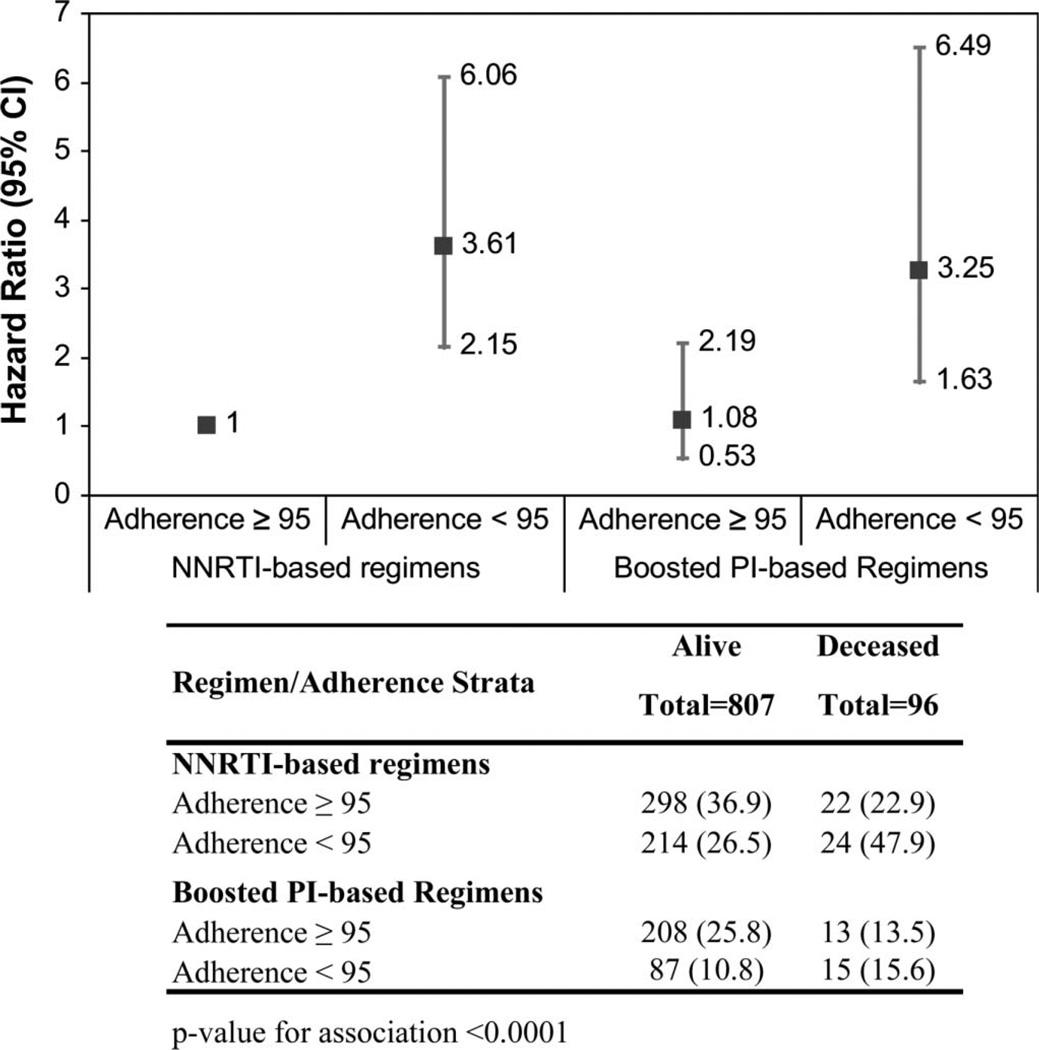
Results: The all-cause mortality was 11%. Individual adherence decreased significantly over time, with the mean adherence shifting from 79% within the first 6 months of starting HAART to 72% within the 24- to 30-month period (P value <0.01). Nonadherence over time (<95%) was strongly associated with higher risk of mortality (hazard ratio: 3.13; 95% confidence interval (CI): 1.95 to 5.05). Nonadherent (<95%) patients on nonnucleoside reverse transcriptase inhibitor (NNRTI)-based and boosted protease inhibitor-based regimens were, respectively, 3.61 times (95% CI: 2.15 to 6.06) and 3.25 times (95% CI: 1.63 to 6.49) more likely to die than adherent patients. Within the NNRTI-based regimens, nonadherent individuals on efavirenz were at a higher risk of mortality.
Conclusions: Incomplete adherence to modern HAART over time was strongly associated with increased mortality, and patients on efavirenz-based NNRTI therapies were particularly at a higher risk if nonadherent. These results highlight the need to develop further strategies to help sustain high levels of adherence on a long-term basis.
Conflict of interest statement
V.D.L. and B.Y. declare no conflict.
Figures
References
-
- Hogg RS, Heath KV, Yip B, et al. Improved survival among HIV-infected individuals following initiation of antiretroviral therapy. JAMA. 1998;279:450–454. - PubMed
-
- Moore RD, Chaisson RE. Natural history of HIV infection in the era of combination antiretroviral therapy. AIDS. 1999;13:1933–1942. - PubMed
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med. 1998;338:853–860. - PubMed
-
- Wood E, Hogg RS, Harrigan PR, et al. When to initiate antiretroviral therapy in HIV-1-infected adults: a review for clinicians and patients. Lancet Infect Dis. 2005;5:407–414. - PubMed
-
- Knobel H, Carmona A, Grau S, et al. Adherence and effectiveness of highly active antiretroviral therapy. Arch Intern Med. 1998;158:1953. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
