

The primary hyperoxalurias
- PMID: 19225556
- PMCID: PMC4577278
- DOI: 10.1038/ki.2009.32
The primary hyperoxalurias
Abstract
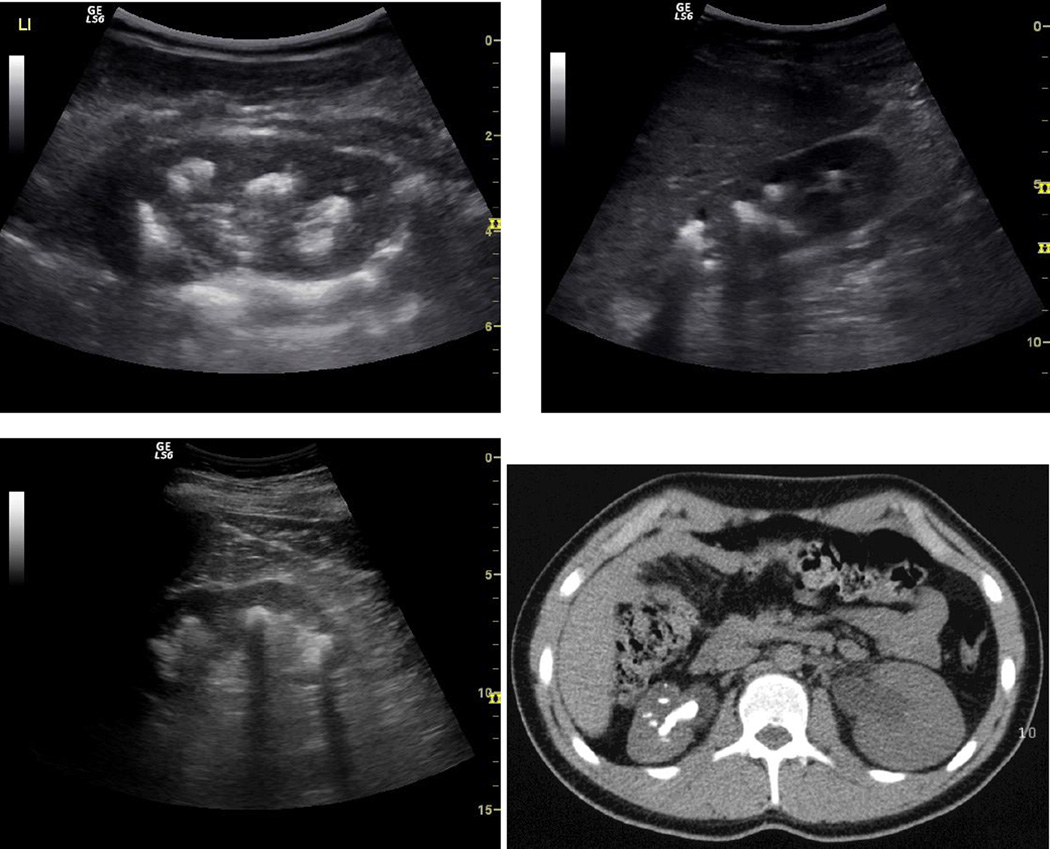
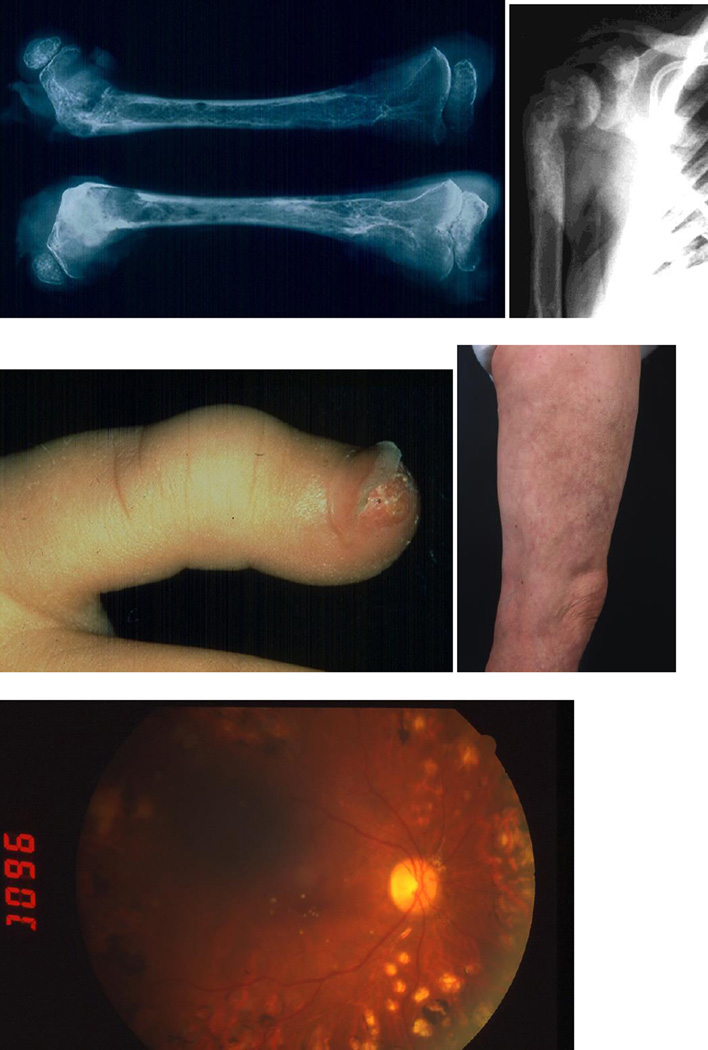
The primary hyperoxalurias (PHs) are rare disorders of glyoxylate metabolism in which specific hepatic enzyme deficiencies result in overproduction of oxalate. Due to the resulting severe hyperoxaluria, recurrent urolithiasis or progressive nephrocalcinosis are principal manifestations. End stage renal failure frequently occurs and is followed by systemic oxalate deposition along with its devastating effects. Due to the lack of familiarity with PHs and their heterogeneous clinical expressions, the diagnosis is often delayed until there is advanced disease. In recent years, improvements in medical management have been associated with better patient outcomes. Although there are several therapeutic options that can help prevent early kidney failure, the only curative treatment to date is combined liver-kidney transplantation in patients with type I PH. Promising areas of investigation are being identified. Knowledge of the spectrum of disease expression, early diagnosis, and initiation of treatment before renal failure are essential to realize a benefit for patients.
Figures
References
-
- Danpure CJ. Primary hyperoxaluria: from gene defects to designer drugs. Nephrol Dial Transplant. 2005;20:1525–1529. - PubMed
-
- Cregeen DP, Williams EL, Hulton S, Rumsby G. Molecular analysis of the glyoxylate reductase (GRHPR) gene and description of mutations underlying primary hyperoxaluria type 2. Hum Mutat. 2003;22:497–506. - PubMed
-
- Monico CG, Persson M, Ford GC, Rumsby G, Milliner DS. Potential mechanisms of marked hyperoxaluria not due to primary hyperoxaluria I or II. Kidney Int. 2002;62:392–400. - PubMed
-
- Leumann E, Hoppe B. The primary hyperoxalurias. J Am Soc Nephrol. 2001;12:1986–1993. - PubMed
-
- Sikora P, von Unruh GE, Beck B, Feldkötter M, Zajaczkowska M, Hesse A, Hoppe B. [13C2]oxalate absorption in children with idiopathic calcium oxalate urolithiasis or primary hyperoxaluria. Kidney Int. 2008;73:1181–1186. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
