

C2-fractures: part I. Quantitative morphology of the C2 vertebra is a prerequisite for the radiographic assessment of posttraumatic C2-alignment and the investigation of clinical outcomes
- PMID: 19225813
- PMCID: PMC2899576
- DOI: 10.1007/s00586-009-0900-5
C2-fractures: part I. Quantitative morphology of the C2 vertebra is a prerequisite for the radiographic assessment of posttraumatic C2-alignment and the investigation of clinical outcomes
Abstract
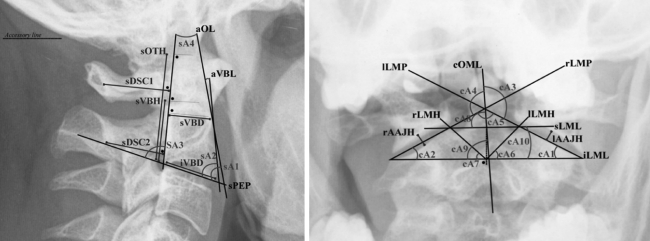
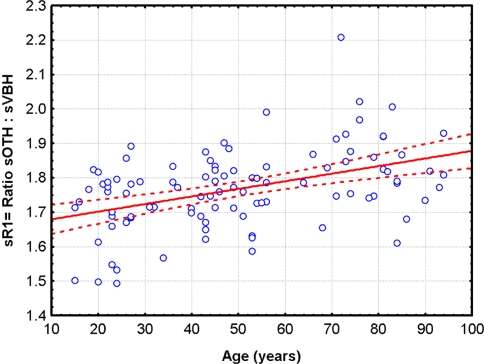
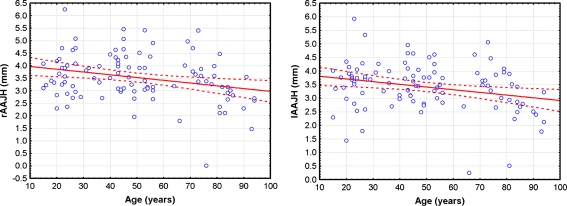
Pertinent literature exists concerning indications, techniques, complications of treatment, and risk factors for nonunion in axis and odontoid fractures; however, there are scarce data regarding the incidence and definition of malunion in these fractures. As a prerequisite for the study of anatomical alignment following surgical and nonsurgical treatment of C2-fractures, an understanding of normal C2 anatomy is essential. Therefore, the authors intended to evaluate morphometrical dimensions of the C2 vertebra. The purpose was to provide normalized quantitative data to enable assessment of malalignment following the treatment of C2-fractures within a classification system. Using digitized cervical spine lateral and transoral odontoid radiographs of 100 consecutive patients without any evidence of traumatic or neoplastic disorders, the authors performed measurements on distinct anatomical structures and investigated morphometrical dimensions of the normal axis vertebra. The incidence of atlantoaxial arthritis was also evaluated. In addition, with the assessment of twenty arbitrarily chosen sets of radiographs by three different observers we calculated the interobserver reliability in terms of intraclass correlation coefficients for each parameter. With calculation of SD and 95% confidence limits, pathological cut-offs were reconstructed from measurements performed resembling non-physiological and pathological limits. Distinct parameters were selected to form a new classification system for radiographical follow-up that focuses on the quantitative C1-2 vertebral alignment. The measurement process resulted in 2,400 data points. Distinct morphometrical parameters, such as a quantitative characterization of the sagittal atlantoaxial congruency, the lateral mass inclination and the type of degenerative changes at the atlantoaxial joint could be demonstrated to be valuable and reliably used within a proposed classification for C2-malunions following C2-fractures. The current study offers a template including recommended radiological measurements for further research on the study of clinical outcome and posttraumatic alignment following C2-fractures.
Figures



References
-
- Blauth M, Richter M, Lange U. Transarticular screw fixation C1/C2 in traumatic atlantoaxial instabilities. Comparison between percutaneous and open procedures. Orthopade. 1999;28:651–661. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
