

Tissue engineering: state of the art in oral rehabilitation
- PMID: 19228277
- PMCID: PMC2744808
- DOI: 10.1111/j.1365-2842.2009.01939.x
Tissue engineering: state of the art in oral rehabilitation
Abstract
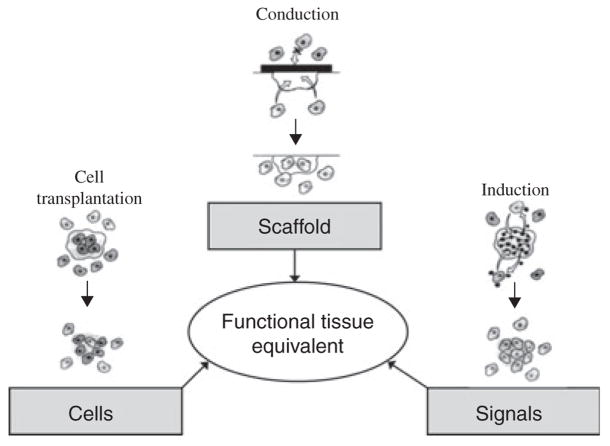
More than 85% of the global population requires repair or replacement of a craniofacial structure. These defects range from simple tooth decay to radical oncologic craniofacial resection. Regeneration of oral and craniofacial tissues presents a formidable challenge that requires synthesis of basic science, clinical science and engineering technology. Identification of appropriate scaffolds, cell sources and spatial and temporal signals (the tissue engineering triad) is necessary to optimize development of a single tissue, hybrid organ or interface. Furthermore, combining the understanding of the interactions between molecules of the extracellular matrix and attached cells with an understanding of the gene expression needed to induce differentiation and tissue growth will provide the design basis for translating basic science into rationally developed components of this tissue engineering triad. Dental tissue engineers are interested in regeneration of teeth, oral mucosa, salivary glands, bone and periodontium. Many of these oral structures are hybrid tissues. For example, engineering the periodontium requires growth of alveolar bone, cementum and the periodontal ligament. Recapitulation of biological development of hybrid tissues and interfaces presents a challenge that exceeds that of engineering just a single tissue. Advances made in dental interface engineering will allow these tissues to serve as model systems for engineering other tissues or organs of the body. This review will begin by covering basic tissue engineering principles and strategic design of functional biomaterials. We will then explore the impact of biomaterials design on the status of craniofacial tissue engineering and current challenges and opportunities in dental tissue engineering.
Figures


References
-
- Laurell L, Gottlow J, Zybutz M, Persson R. Treatment of intrabony defects by different surgical procedures. A literature review. J Periodontol. 1998;69:303–313. - PubMed
-
- Phillips JH, Forrest CR, Gruss JS. Current concepts in the use of bone grafts in facial fractures. Basic science considerations. Clin Plast Surg. 1992;19:41–58. - PubMed
-
- Kashi A, Saha S, Christensen RW. Temporomandibular joint disorders: artificial joint replacements and future research needs. J Long Term Eff Med Implants. 2006;16:459–474. - PubMed
-
- Garcia-Godoy F, Murray PE. Status and potential commercial impact of stem cell-based treatments on dental and craniofacial regeneration. Stem Cells Dev. 2006;15:881–887. - PubMed
-
- Aframian DJ, Palmon A. Current status of the development of an artificial salivary gland. Tissue Eng. 2008;14:187–198. - PubMed
