

The last man standing is the most resistant: eliminating artemisinin-resistant malaria in Cambodia
- PMID: 19228438
- PMCID: PMC2660356
- DOI: 10.1186/1475-2875-8-31
The last man standing is the most resistant: eliminating artemisinin-resistant malaria in Cambodia
Abstract
Background: Artemisinin combination therapy (ACT) is now the recommended first-line treatment for falciparum malaria throughout the world. Initiatives to eliminate malaria are critically dependent on its efficacy. There is recent worrying evidence that artemisinin resistance has arisen on the Thai-Cambodian border. Urgent containment interventions are planned and about to be executed. Mathematical modeling approaches to intervention design are now integrated into the field of malaria epidemiology and control. The use of such an approach to investigate the likely effectiveness of different containment measures with the ultimate aim of eliminating artemisinin-resistant malaria is described.
Methods: A population dynamic mathematical modeling framework was developed to explore the relative effectiveness of a variety of containment interventions in eliminating artemisinin-resistant malaria in western Cambodia.
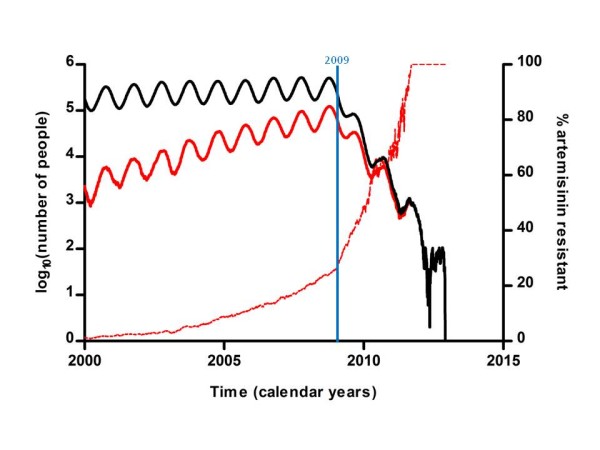
Results: The most effective intervention to eliminate artemisinin-resistant malaria was a switch of treatment from artemisinin monotherapy to ACT (mean time to elimination 3.42 years (95% CI 3.32-3.60 years). However, with this approach it is predicted that elimination of artemisinin-resistant malaria using ACT can be achieved only by elimination of all malaria. This is because the various forms of ACT are more effective against infections with artemisinin-sensitive parasites, leaving the more resistant infections as an increasing proportion of the dwindling parasite population.
Conclusion: Containment of artemisinin-resistant malaria can be achieved by elimination of malaria from western Cambodia using ACT. The "last man standing" is the most resistant and thus this strategy must be sustained until elimination is truly achieved.
Figures



References
-
- Verdrager J. Epidemiology of the emergence and spread of drug-resistant falciparum malaria in South-East Asia and Australasia. J Trop Med Hyg. 1986;89:277–289. - PubMed
-
- Bosman A, Mendis KN. A major transition in malaria treatment: the adoption and deployment of artemisinin-based combination therapies. Am J Trop Med Hyg. 2007;77:193–197. - PubMed
-
- Global Malaria Programme. World Health Organization; 2006. WHO guidelines for the treatment of malaria.http://www.who.int/malaria/docs/TreatmentGuidelines2006.pdf
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
