

Comparison of threshold cutpoints and continuous measures of anti-cyclic citrullinated peptide antibodies in predicting future rheumatoid arthritis
- PMID: 19228654
- PMCID: PMC3108039
- DOI: 10.3899/jrheum.080895
Comparison of threshold cutpoints and continuous measures of anti-cyclic citrullinated peptide antibodies in predicting future rheumatoid arthritis
Abstract
Objective: Anti-cyclic citrullinated peptide (anti-CCP) antibodies are strongly associated with increased risk of rheumatoid arthritis (RA).While the anti-CCP level is commonly dichotomized for clinical use, the best threshold for and utility of the titer as a continuous variable to predict development of RA are uncertain.
Methods: Using data from the Nurses' Health Study and Nurses' Health Study II longitudinal cohorts, we examined the sensitivity, specificity, and hazard of RA at various thresholds of the anti-CCP. Incident RA was confirmed using the Connective Tissue Disease Screening Questionnaire and medical record review in 93 women from among 62,437 participants with blood samples. Three controls per case were randomly chosen, matching on cohort, age, and menopausal status. Stored plasma was tested for anti-CCP antibodies with the second-generation Diastat ELISA. Five threshold values were assessed for sensitivity, specificity, and time to diagnosis of RA. Hazard of RA was assessed with conditional logistic regression models adjusting for smoking and reproductive factors.
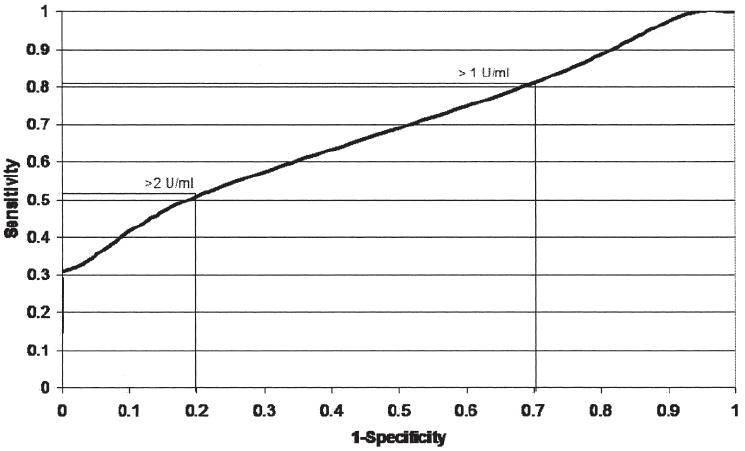
Results: Using the suggested threshold of >5 U/ml for anti-CCP positivity, specificity was 100%, but sensitivity was only 28%. A threshold of >2 U/ml had a higher sensitivity (51%), and similar specificity (80%), with an odds ratio of 11.2 (95% confidence interval 4.7-26.9) for RA. Anti-CCP level as an ordinal variable was strongly associated with time to RA onset, with higher values predicting shorter time to RA onset.
Conclusion: A lower threshold for anti-CCP positivity was more sensitive in predicting RA development. Higher ranges of the level were informative in predicting time to RA onset.
Figures
Comment in
-
Anti-cyclic citrullinated peptide in preclinical rheumatoid arthritis. Food for thought.J Rheumatol. 2009 Apr;36(4):663-4. doi: 10.3899/jrheum.090184. J Rheumatol. 2009. PMID: 19342718 No abstract available.
-
Low level (below cutoff) of anti-cyclic citrullinated peptide test results in diagnosis of rheumatoid arthritis in a high-risk population.J Rheumatol. 2010 Jan;37(1):208. doi: 10.3899/jrheum.090555. J Rheumatol. 2010. PMID: 20040646 No abstract available.
References
-
- Pincus T, Callahan LF, Sale WG, Brooks AL, Payne LE, Vaughn WK. Severe functional declines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over nine years. Arthritis Rheum. 1984;27:864–72. - PubMed
-
- Smolen JS, Han C, van der Heijde D, et al. Infliximab treatment maintains employability in patients with early rheumatoid arthritis. Arthritis Rheum. 2006;54:716–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources