

Impact of plaque components on no-reflow phenomenon after stent deployment in patients with acute coronary syndrome: a virtual histology-intravascular ultrasound analysis
- PMID: 19228713
- PMCID: PMC3155758
- DOI: 10.1093/eurheartj/ehp034
Impact of plaque components on no-reflow phenomenon after stent deployment in patients with acute coronary syndrome: a virtual histology-intravascular ultrasound analysis
Abstract
Aims: We used virtual histology-intravascular ultrasound (VH-IVUS) to evaluate the relation between coronary plaque characteristics and no-reflow in acute coronary syndrome (ACS) patients.
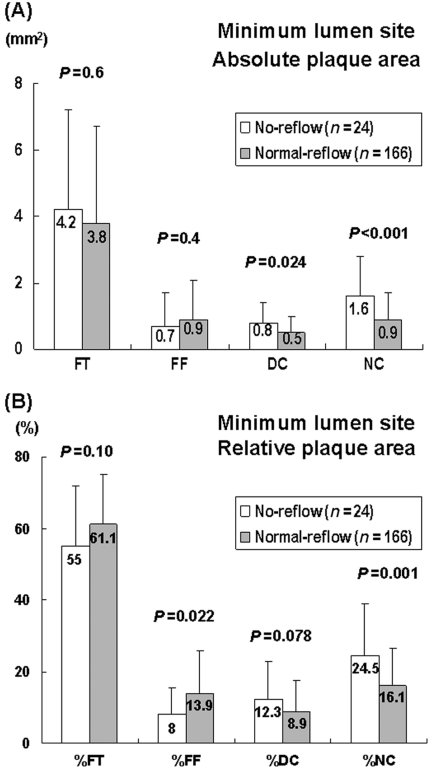
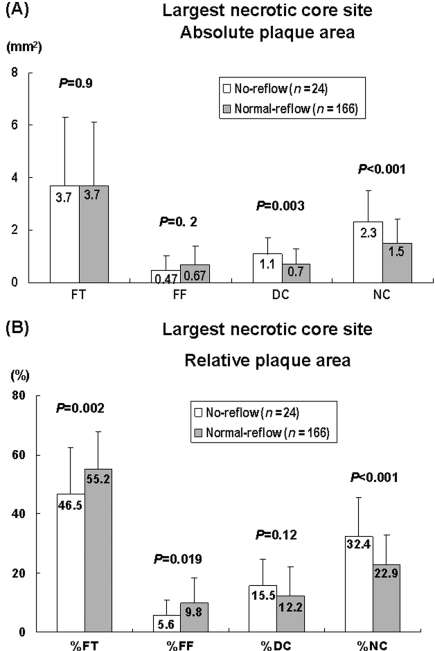
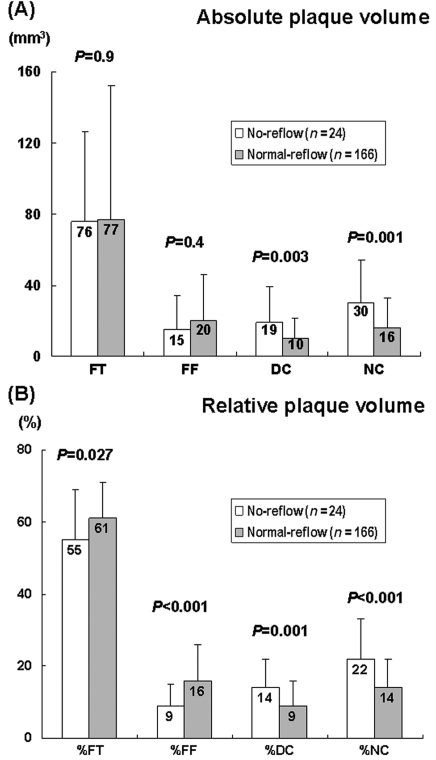
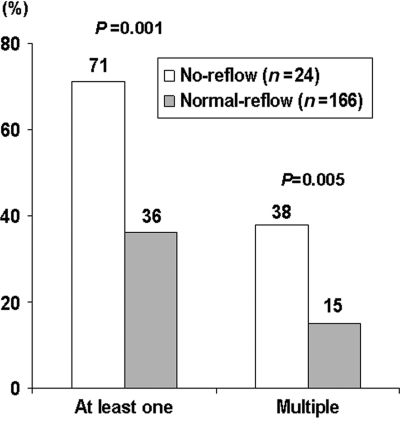
Methods and results: A total of 190 consecutive ACS patients were imaged using VH-IVUS and analysed retrospectively. Angiographic no-reflow was defined as TIMI flow grade 0, 1, and 2 after stenting. Virtual histology-intravascular ultrasound classified the colour-coded tissue into four major components: fibrotic, fibro-fatty, dense calcium, and necrotic core (NC). Thin-cap fibroatheroma (TCFA) was defined as focal, NC-rich (≥10% of the cross-sectional area) plaques being in contact with the lumen in a plaque burden≥40%. Of the 190 patients studied at pre-stenting, no-reflow was observed in 24 patients (12.6%) at post-stenting. The absolute and %NC areas at the minimum lumen sites (1.6±1.2 vs. 0.9±0.8 mm2, P<0.001, and 24.5±14.3 vs. 16.1±10.6%, P=0.001, respectively) and the absolute and %NC volumes (30±24 vs. 16±17 mm3, P=0.001, and 22±11 vs. 14±8%, P<0.001, respectively) were significantly greater, and the presence of at least one TCFA and multiple TCFAs within culprit lesions (71 vs. 36%, P=0.001, and 38 vs. 15%, P=0.005, respectively) was significantly more common in the no-reflow group compared with the normal-reflow group. In the multivariable analysis, %NC volume was the only independent predictor of no-reflow (odds ratio=1.126; 95% CI 1.045-1.214, P=0.002).
Conclusion: In ACS patients, post-stenting no-reflow is associated with plaque components defined by VH-IVUS analysis with larger NC and more TCFAs.
Figures
References
-
- Weaver WD, Simes RJ, Betriu A, Grines CL, Zijlstra F, Garcia E, Grinfeld L, Gibbons RJ, Ribeiro EE, DeWood MA, Ribichini F. Comparison of primary coronary angioplasty and intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review. A meta analysis. JAMA. 1997;278:2093–2098. - PubMed
-
- Suryapranata H, van ‘t Hof AW, Hoorntje JC, de Boer MJ, Zijlstra F. Randomized comparison of coronary stenting with balloon angioplasty in selected patients with acute myocardial infarction. Circulation. 1998;97:2502–2505. - PubMed
-
- Mahdi NA, Lopez J, Leon M, Pathan A, Harrell L, Jang IK, Palacios IF. Comparison of coronary stenting to primary balloon angioplasty with stent bail out for the treatment of patients with acute myocardial infarction. Am J Cardiol. 1998;81:957–963. - PubMed
-
- Piana RN, Paik GY, Moscucci M, Cohen DJ, Gibson CM, Kugelmass AD, Carrozza JP, Jr, Kuntz RE, Baim DS. Incidence and treatment of ‘no-reflow’ after percutaneous coronary intervention. Circulation. 1994;89:2514–2518. - PubMed
-
- Morishima I, Sone T, Mokuno S, Taga S, Shimauchi A, Oki Y, Kondo J, Tsuboi H, Sassa H. Clinical significance of no-reflow phenomenon observed on angiography after successful treatment of acute myocardial infarction with percutaneous transluminal coronary angioplasty. Am Heart J. 1995;130:239–243. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
