

Hand-foot skin reaction increases with cumulative sorafenib dose and with combination anti-vascular endothelial growth factor therapy
- PMID: 19228742
- PMCID: PMC2718558
- DOI: 10.1158/1078-0432.CCR-08-1141
Hand-foot skin reaction increases with cumulative sorafenib dose and with combination anti-vascular endothelial growth factor therapy
Abstract
Purpose: Sorafenib, a vascular endothelial growth factor (VEGF) receptor-2 and RAF kinase inhibitor, commonly causes skin toxicity. We retrospectively analyzed dermatologic toxicity in patients receiving combined antiangiogenic therapy involving sorafenib and bevacizumab.
Experimental design: Castration-resistant prostate cancer and metastatic non-small cell lung cancer patients were accrued to phase II studies, receiving sorafenib 400 mg twice daily. A phase I study explored sorafenib 200 to 400 mg twice daily with bevacizumab 5 to 10 mg/kg every 2 weeks in patients with advanced solid tumors. The probability of development of maximum grade of dermatologic toxicity as a function of the cumulative dose of sorafenib was determined. Additional analyses compared extent of toxicity, pharmacokinetics, and patient risk factors.
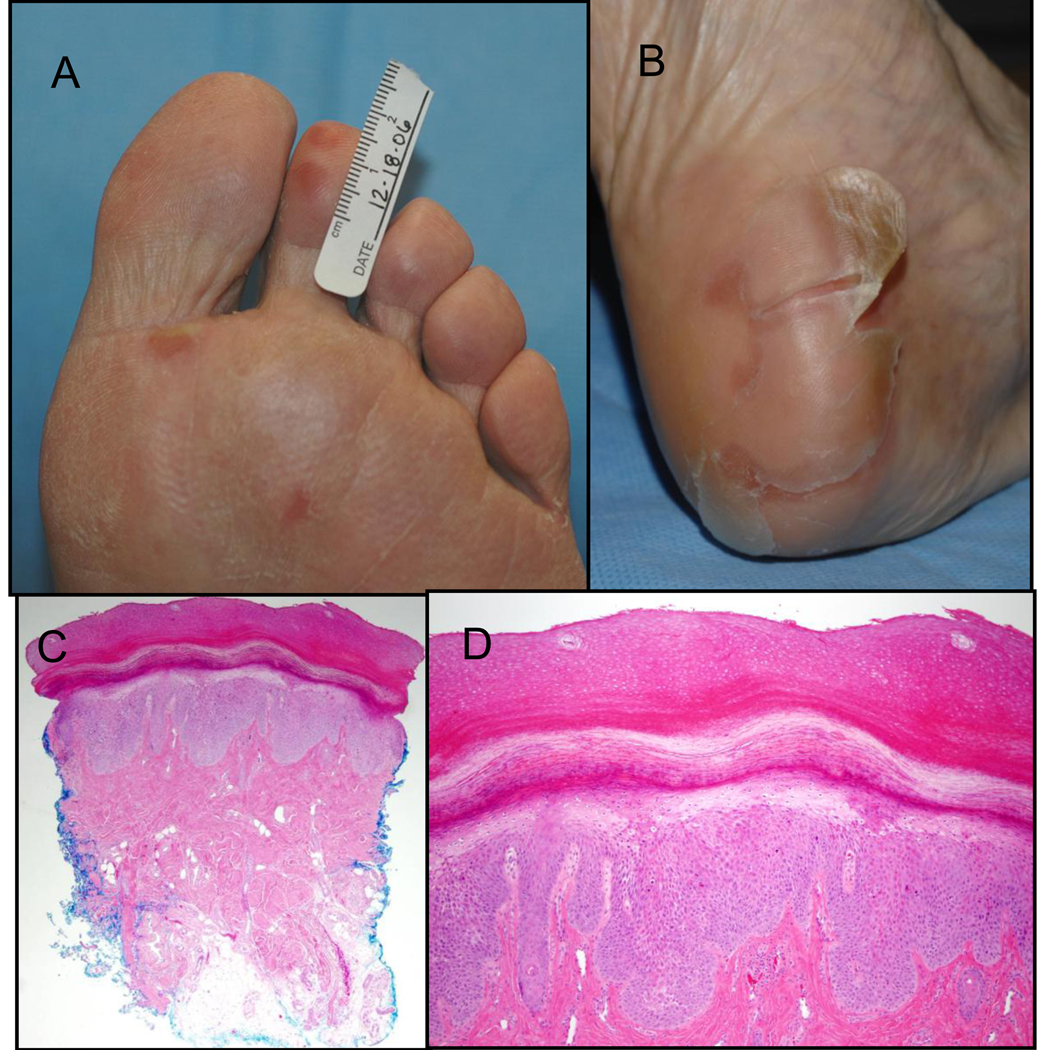
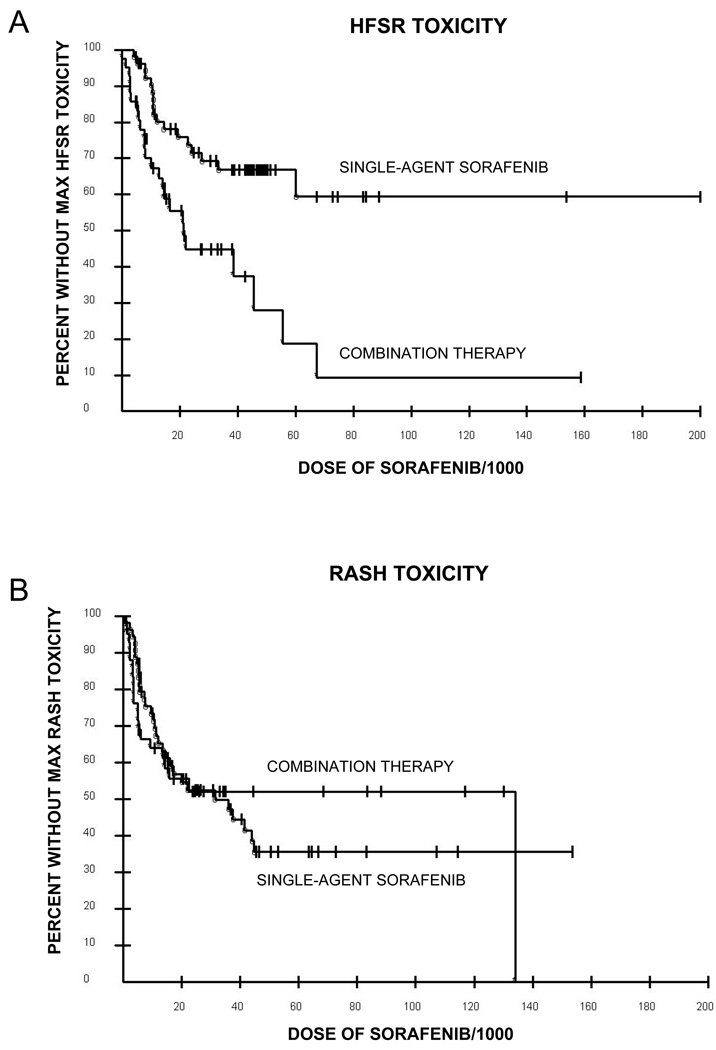
Results: Ninety-six patients were enrolled: 54 received sorafenib and 42 received bevacizumab/sorafenib. Hand-foot skin reaction (HFSR) was observed in 50 of 96 (52%) patients. Grade 2 to 3 HFSR developed in 16 of 54 (30%) sorafenib patients and 24 of 42 (57%) bevacizumab/sorafenib patients (P=0.012) and was associated with cumulative sorafenib exposure (P=0.0008). Twenty-four of 42 phase I patients randomized to start with bevacizumab had increased risk of grade 2 to 3 HFSR than those starting with sorafenib (P=0.013) after adjusting for association between HFSR risk and hypertension (P=0.01), which was the only toxicity associated with HFSR. There was no association between HFSR and baseline history of neuropathy, prior taxane/platinum treatment, or systemic sorafenib levels.
Conclusions: Sorafenib-related HFSR is associated with increasing cumulative sorafenib dose. HFSR is increased in patients treated with bevacizumab/sorafenib combination anti-VEGF therapy, and this finding is not explained by pharmacokinetic interaction between the two agents. Our results suggest that the pathophysiology of HFSR may be related to VEGF inhibition.
Conflict of interest statement
Figures
References
-
- Lokich JJ, Moore C. Chemotherapy-associated palmar-plantar erythrodysesthesia syndrome. Ann Intern Med. 1984;101:798–799. - PubMed
-
- Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med. 2004;351:337–345. - PubMed
-
- Lai SE, Kuzel T, Lacouture ME. Hand-foot and stump syndrome to sorafenib. J Clin Oncol. 2007;25:341–343. - PubMed
-
- Kane RC, Farrell AT, Saber H, et al. Sorafenib for the treatment of advanced renal cell carcinoma. Clin Cancer Res. 2006;12:7271–7278. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
