

Brain metastasis from an unknown primary, or primary brain tumour? A diagnostic dilemma
- PMID: 19229374
- PMCID: PMC2644621
- DOI: 10.3747/co.v16i1.308
Brain metastasis from an unknown primary, or primary brain tumour? A diagnostic dilemma
Abstract
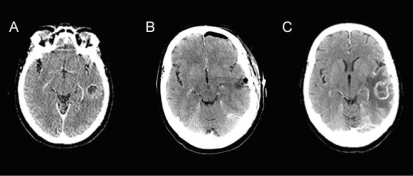
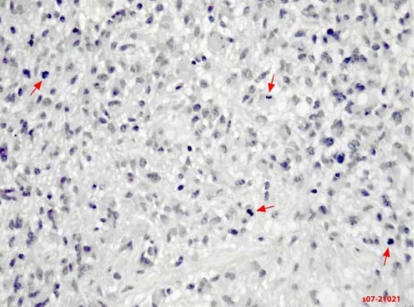
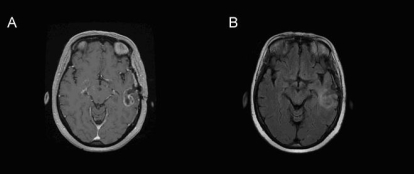
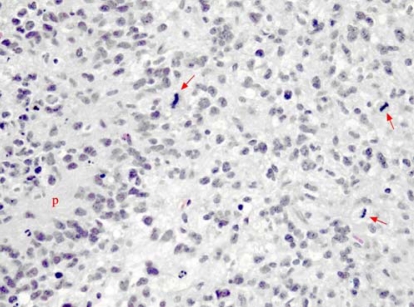
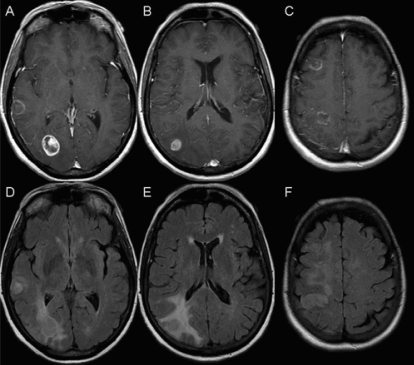
Brain metastasis is increasingly common, affecting 20%-40% of cancer patients. After diagnosis, survival is usually limited to months in these patients. Treatment for brain metastasis includes whole-brain radiation therapy, surgical resection, or both. These treatments aim to slow progression of disease and to improve or maintain neurologic function and quality of life.Although less common, primary brain tumours produce symptoms that are similar to those of brain metastasis. Glioblastoma, the most common malignant tumour of the brain, has a median survival of less than 12 months. Patients are often treated with surgical resection followed by radical radiation therapy and chemotherapy.Here, we present 2 separate cases of lesions in the brain radiologically compatible with brain metastasis. In both cases, no primary cancer site had been established, and neurosurgical intervention was sought to obtain a pathologic diagnosis. Both cases were pathologically confirmed as glioblastoma. These cases demonstrate the importance of differentiation between brain metastases and primary brain tumours to ensure that the appropriate management strategy is implemented.
Keywords: Brain metastasis; glioblastoma multiforme; unknown primary; wbrt; whole-brain radiation therapy.
Figures
References
-
- Kleihues P, Cavenee WK, editors. Pathology and Genetics of Tumours of the Nervous System. 2nd ed. Lyon, France: IARC Press; 2000.
-
- Legler JM, Ries LA, Smith MA, et al. Cancer surveillance series [corrected]: brain and other central nervous system cancers: recent trends in incidence and mortality. J Natl Cancer Inst. 1999;91:1382–90. [Erratum in: J Natl Cancer Inst 1999;91:1693] - PubMed
-
- Behin A, Hoang–Xuan K, Carpentier AF, Delattre JY. Primary brain tumours in adults. Lancet. 2003;361:323–31. - PubMed
-
- Patchell RA. The management of brain metastases. Cancer Treat Rev. 2003;29:533–40. - PubMed
-
- Nussbaum ES, Djalilian HR, Cho KH, Hall WA. Brain metastases. Histology, multiplicity, surgery, and survival. Cancer. 1996;78:1781–8. - PubMed
LinkOut - more resources
Full Text Sources
