

A multi-institutional evaluation of active surveillance for low risk prostate cancer
- PMID: 19233410
- PMCID: PMC4237227
- DOI: 10.1016/j.juro.2008.11.109
A multi-institutional evaluation of active surveillance for low risk prostate cancer
Abstract
Purpose: For select men with low risk prostate cancer active surveillance is more often being considered a management strategy. In a multicenter retrospective study we evaluated the actuarial rates and predictors of remaining on active surveillance, the incidence of cancer progression and the pathological findings of delayed radical prostatectomy.
Materials and methods: A cohort of 262 men from 4 institutions met the inclusion criteria of age 75 years or younger, prostate specific antigen 10 ng/ml or less, clinical stage T1-T2a, biopsy Gleason sum 6 or less, 3 or less positive cores at diagnostic biopsy, repeat biopsy before active surveillance and no treatment for 6 months following the repeat biopsy. Active surveillance started on the date of the second biopsy. Actuarial rates of remaining on active surveillance were calculated and univariate Cox regression was used to assess predictors of discontinuing active surveillance.
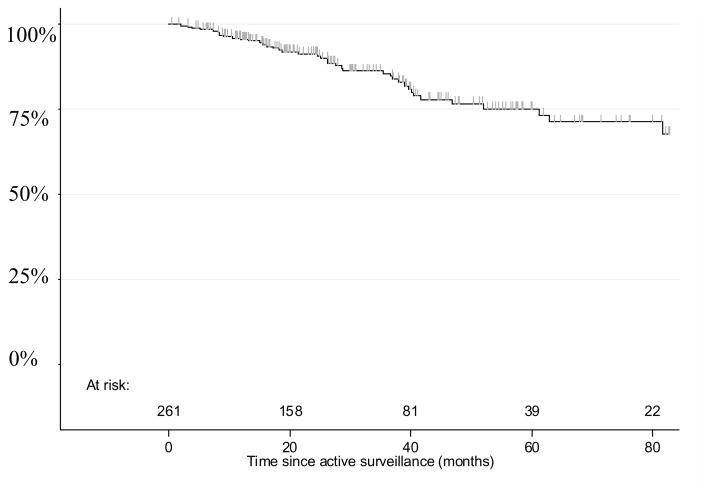
Results: With a median followup of 29 months 43 patients ultimately received active treatment. The 2 and 5-year probabilities of remaining on active surveillance were 91% and 75%, respectively. Patients with cancer on the second biopsy (HR 2.23, 95% CI 1.23-4.06, p = 0.007) and a higher number of cancerous cores from the 2 biopsies combined (p = 0.002) were more likely to undergo treatment. Age, prostate specific antigen, clinical stage, prostate volume and number of total biopsy cores sampled were not predictive of outcome. Skeletal metastases developed in 1 patient 38 months after starting active surveillance. Of the 43 patients undergoing delayed treatment 41 (95%) are without disease progression at a median of 23 months following treatment.
Conclusions: With a median followup of 29 months active surveillance for select patients appears to be safe and associated with a low risk of systemic progression. Cancer at restaging biopsy and a higher total number of cancerous cores are associated with a lower likelihood of remaining on active surveillance. A restaging biopsy should be strongly considered to finalize eligibility for active surveillance.
Figures
Comment in
-
Prostate specific antigen screening and active surveillance in the elderly.J Urol. 2009 Apr;181(4):1534-5. doi: 10.1016/j.juro.2009.01.065. Epub 2009 Feb 23. J Urol. 2009. PMID: 19230925 No abstract available.
-
Re: A multi-institutional evaluation of active surveillance for low risk prostate cancer. S. E. Eggener, A. Mueller, R. K. Berglund, R. Ayyathurai, C. Soloway, M. S. Soloway, R. Abouassaly, E. A. Klein, S. J. Jones, C. Zappavigna, L. Goldenberg, P. T. Scardino, J. A. Eastham and B. Guillonneau J Urol 2009; 181: 1635-1641.J Urol. 2010 Sep;184(3):1223-4; author reply 1224. doi: 10.1016/j.juro.2010.05.001. Epub 2010 Jul 22. J Urol. 2010. PMID: 20655069 No abstract available.
Similar articles
-
A multi-institutional evaluation of active surveillance for low risk prostate cancer.J Urol. 2013 Jan;189(1 Suppl):S19-25; discussion S25. doi: 10.1016/j.juro.2012.11.023. J Urol. 2013. PMID: 23234624
-
Active surveillance for the management of prostate cancer in a contemporary cohort.Cancer. 2008 Jun 15;112(12):2664-70. doi: 10.1002/cncr.23502. Cancer. 2008. PMID: 18433013 Clinical Trial.
-
Active surveillance of very-low-risk prostate cancer in the setting of active treatment of benign prostatic hyperplasia with 5α-reductase inhibitors.Urology. 2013 May;81(5):979-84. doi: 10.1016/j.urology.2012.10.089. Epub 2013 Mar 20. Urology. 2013. PMID: 23523297
-
Optimization of prostate biopsy in patients considered for active surveillance. The role of the confirmatory biopsy and transperineal techniques.Arch Esp Urol. 2014 Jun;67(5):409-18. Arch Esp Urol. 2014. PMID: 24914840 Review. English, Spanish.
-
Identifying intermediate-risk candidates for active surveillance of prostate cancer.Urol Oncol. 2017 Oct;35(10):605.e1-605.e8. doi: 10.1016/j.urolonc.2017.06.048. Epub 2017 Jul 20. Urol Oncol. 2017. PMID: 28736249 Review.
Cited by
-
Prostate-specific antigen test result interpretation when combined with risk factors for recommendation of biopsy: a survey of urologist's practice patterns.Int Urol Nephrol. 2011 Mar;43(1):31-7. doi: 10.1007/s11255-010-9772-1. Epub 2010 Jun 12. Int Urol Nephrol. 2011. PMID: 20544283
-
Prognostic influence of 5 alpha reductase inhibitors in patients with localized prostate cancer under active surveillance.Turk J Urol. 2018 Mar;44(2):132-137. doi: 10.5152/tud.2017.39660. Epub 2018 Mar 1. Turk J Urol. 2018. PMID: 29511582 Free PMC article.
-
In-bore MRI-guided biopsy: can it optimize the need for periodic biopsies in prostate cancer patients undergoing active surveillance? A pilot test-retest reliability study.Br J Radiol. 2018 Apr;91(1084):20170603. doi: 10.1259/bjr.20170603. Epub 2018 Feb 13. Br J Radiol. 2018. PMID: 29308912 Free PMC article.
-
Selecting Active Surveillance: Decision Making Factors for Men with a Low-Risk Prostate Cancer.Med Decis Making. 2019 Nov;39(8):962-974. doi: 10.1177/0272989X19883242. Epub 2019 Oct 21. Med Decis Making. 2019. PMID: 31631745 Free PMC article.
-
Is there an optimal management for localized prostate cancer?Clin Interv Aging. 2010 Aug 9;5:187-97. doi: 10.2147/cia.s6555. Clin Interv Aging. 2010. PMID: 20711438 Free PMC article. Review.
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71. - PubMed
-
- Roemeling S, Roobol MJ, Kattan MW, van der Kwast TH, Steyerberg EW, Schroder FH. Nomogram use for the prediction of indolent prostate cancer: impact on screen-detected populations. Cancer. 2007;110:2218. - PubMed
-
- Dall'Era MA, Cooperberg MR, Chan JM, Davies BJ, Albertsen PC, Klotz LH, et al. Active surveillance for early-stage prostate cancer: review of the current literature. Cancer. 2008;112:1650. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
