

Assessment of liver fibrosis by transient elastography in persons with hepatitis C virus infection or HIV-hepatitis C virus coinfection
- PMID: 19236273
- PMCID: PMC2715996
- DOI: 10.1086/597350
Assessment of liver fibrosis by transient elastography in persons with hepatitis C virus infection or HIV-hepatitis C virus coinfection
Abstract
Background: Transient elastography is a novel, noninvasive method for staging liver fibrosis. We compared elastography with histologic methods among hepatitis C virus (HCV)-infected and human immunodeficiency virus (HIV)-HCV-coinfected participants in an urban, predominantly black study population.
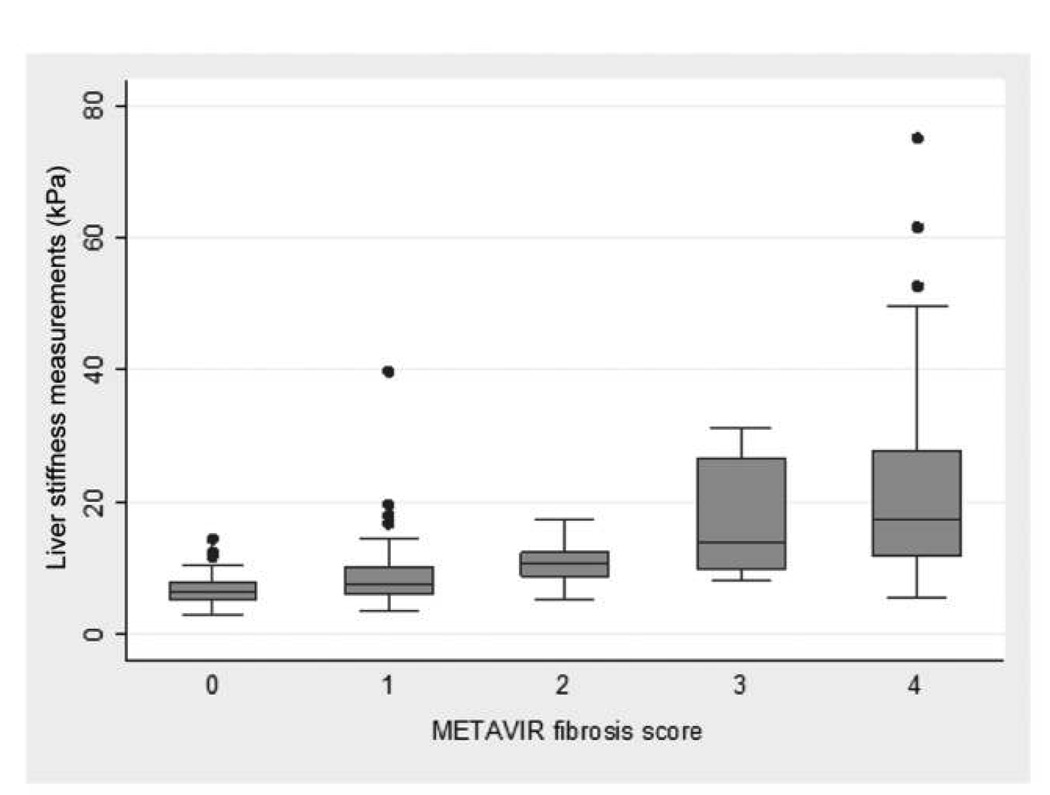
Methods: Participants recruited from the AIDS Linked to the Intravenous Experience and the Johns Hopkins HIV Clinical Cohort studies underwent elastography to determine liver stiffness measurements. Liver biopsy specimens were staged F0-F4 in accordance with the Metavir score. Diagnostic accuracy and determination of liver stiffness cutoff values, compared with histologic methods, were determined by receiver operating characteristic analysis. Logistic regression methods identified parameters associated with discordant classification status.
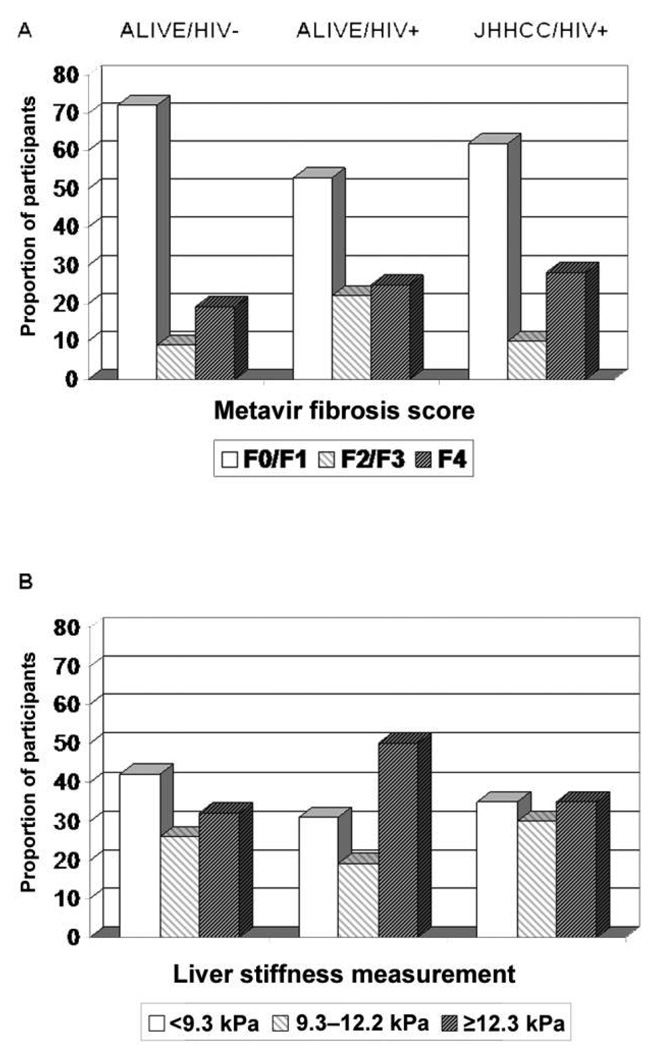
Results: Of 192 participants, 139 (72%) were coinfected with HIV and HCV, 121 (63%) had insignificant fibrosis, and 48 (25%) had cirrhosis. Overall, the area-under-the-curve receiver operating characteristic was 0.87 for detection of both significant fibrosis (95% confidence interval, 0.82-0.92) and cirrhosis (95% confidence interval, 0.81-0.93). With use of cutoff values of 9.3 kPa for fibrosis and 12.3 kPa for cirrhosis, 79%-83% of participants were correctly classified by liver stiffness measurement (compared with histologic methods); accuracy appeared to be higher among HIV-uninfected participants than among HIV-infected participants. Most discordance occurred when liver stiffness measurements indicated liver disease and histologic examination did not (in 16% of participants); the patients with these discordant results were more likely to have attributes that increased the odds of significant fibrosis, such as elevated serum fibrosis markers or HIV-related immunosuppression, compared with persons in whom low fibrosis was predicted by both examination of a biopsy specimen and elastography.
Conclusions: For most HCV-infected persons, fibrosis stage predicted by elastography is similar to that predicted by examination of a biopsy specimen. Elastography-based measurement of liver stiffness holds promise to expand liver disease screening and monitoring, particularly among injection drug users.
Conflict of interest statement
Figures
References
-
- Benhamou Y, Bochet M, Di Martino V, et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. The Multivirc Group. Hepatology. 1999;30:1054–1058. - PubMed
-
- Goedert JJ, Eyster ME, Lederman MM, et al. End-stage liver disease in persons with hemophilia and transfusion-associated infections. Blood. 2002;100:1584–1589. - PubMed
-
- Weber R, Sabin CA, Friis-Moller N, et al. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D study. Arch Intern Med. 2006;166:1632–1641. - PubMed
-
- Bedossa P, Dargere D, Paradis V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology. 2003;38:1449–1457. - PubMed
-
- Regev A, Berho M, Jeffers LJ, et al. Sampling error and intraobserver variation in liver biopsy in patients with chronic HCV infection. Am J Gastroenterol. 2002;97:2614–2618. - PubMed
Publication types
MeSH terms
Grants and funding
- R56 DA004334/DA/NIDA NIH HHS/United States
- R01 DA004334/DA/NIDA NIH HHS/United States
- DA04334/DA/NIDA NIH HHS/United States
- DA13806/DA/NIDA NIH HHS/United States
- R01 DA016078/DA/NIDA NIH HHS/United States
- R56 DA012568/DA/NIDA NIH HHS/United States
- R01S DA16078/DA/NIDA NIH HHS/United States
- R21 AA015032/AA/NIAAA NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- DA12568/DA/NIDA NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- R01 DA013806/DA/NIDA NIH HHS/United States
- UL1RR025005/RR/NCRR NIH HHS/United States
- R01 AA016893/AA/NIAAA NIH HHS/United States
- R37 DA004334/DA/NIDA NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- R37 DA013806/DA/NIDA NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- K24 DA000432/DA/NIDA NIH HHS/United States
- U01 DA036935/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
