

Implanted electrical stimulation of the trunk for seated postural stability and function after cervical spinal cord injury: a single case study
- PMID: 19236990
- PMCID: PMC2648134
- DOI: 10.1016/j.apmr.2008.07.029
Implanted electrical stimulation of the trunk for seated postural stability and function after cervical spinal cord injury: a single case study
Abstract
Objectives: To explore and quantify the physical and functional effects of stabilizing the torso with electrical stimulation of the paralyzed hip and trunk musculature after motor complete tetraplegia.
Design: Single-subject case study with repeated measures and concurrent controls.
Setting: Academic outpatient rehabilitation center.
Participants: Forty-four-year-old man with C4 American Spinal Injury Association grade A tetraplegia 20 years postspinal cord injury.
Intervention: A surgically implanted multichannel pulse generator and intramuscular stimulating electrodes to activate lumbar erector spinae, quadratus lumborum, and gluteus maximus muscles bilaterally.
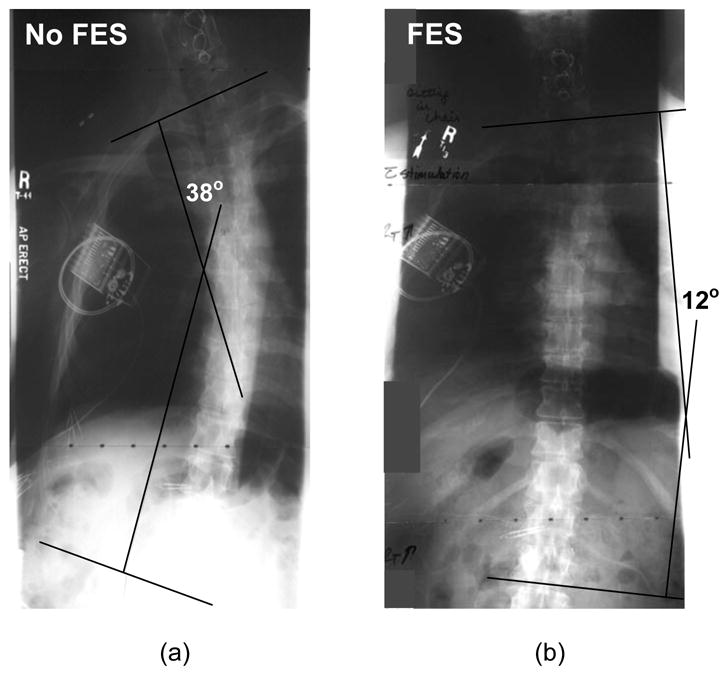
Main outcome measures: Outcomes assessed with and without stimulation included (1) spinal alignment and pelvic orientation, (2) pulmonary function and ventilatory volumes, (3) forward bimanual reaching distance, (4) seated stability and resistance to externally applied disturbances, (5) maximal force and speed of rowing-like movements, and the ability to (6) independently return to an erect seated position from full forward or lateral flexion and (7) roll in bed without assistance.
Results: Stimulation improved spinal convexity and kyphosis by 26 degrees and 21 degrees , reduced posterior pelvic tilt by 11 degrees , increased forced expiratory volume and vital capacity by 10% and 22%, and improved forward reach by more than 7cm. Average resistance to sagittal disturbances increased by more than 40% (P<.002), and mean force exerted during underhanded pulling more than doubled (P=.014) with stimulation. Restoration of upright sitting in both sagittal and coronal planes and bed turning was made possible through appropriately timed activation of the hip and trunk muscles.
Conclusions: A neuroprosthesis for controlling the paralyzed torso can positively impact spinal alignment, seated posture, pulmonary function, trunk stability, and reach. Stimulation of hip and trunk muscles can improve performance of activities of daily living as well as enable independent wheelchair and bed mobility.
Figures




References
-
- Sinnott KA, Milburn P, McNaughton H. Factors associated with thoracic spinal cord injury, lesion level and rotator cuff disorders. Spinal Cord. 2000;38:748–53. - PubMed
-
- Anderson K. Targeting recovery: Priorities of the spinal cord injured population. Journal of Neurotrauma. 2004;21:1371–83. - PubMed
-
- Brown-Triolo DL, Roach ML, Triolo RJ, Nelson K. Consumer perspectives on mobility: implications for neuroprosthesis design. Journal of Rehabilitation Research & Development. 2002;39:659–69. - PubMed
-
- Bogie KM, Wang X, Triolo RJ. Long term prevention of pressure ulcers in high-risk individuals: a case study of the use of gluteal neuromuscular electrical stimulation. Arch Phys Med &Rehab. 2006;87:585–91. - PubMed
-
- Bogie K, Triolo RJ. The effects of regular use of neuromuscular electrical stimulation on tissue health. Journal of Rehabilitation Research & Development. 2003;40:469–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
