

Dairy food, calcium, and risk of cancer in the NIH-AARP Diet and Health Study
- PMID: 19237724
- PMCID: PMC2796799
- DOI: 10.1001/archinternmed.2008.578
Dairy food, calcium, and risk of cancer in the NIH-AARP Diet and Health Study
Abstract
Background: Dairy food and calcium intakes have been hypothesized to play roles that differ among individual cancer sites, but the evidence has been limited and inconsistent. Moreover, their effect on cancer in total is unclear.
Methods: Dairy food and calcium intakes in relation to total cancer as well as cancer at individual sites were examined in the National Institutes of Health (NIH)-AARP (formerly known as the American Association of Retired Persons) Diet and Health Study. Intakes of dairy food and calcium from foods and supplements were assessed with a food frequency questionnaire. Incident cancer cases were identified through linkage with state cancer registries. A Cox proportional hazard model was used to estimate relative risks and 2-sided 95% confidence intervals (CIs).
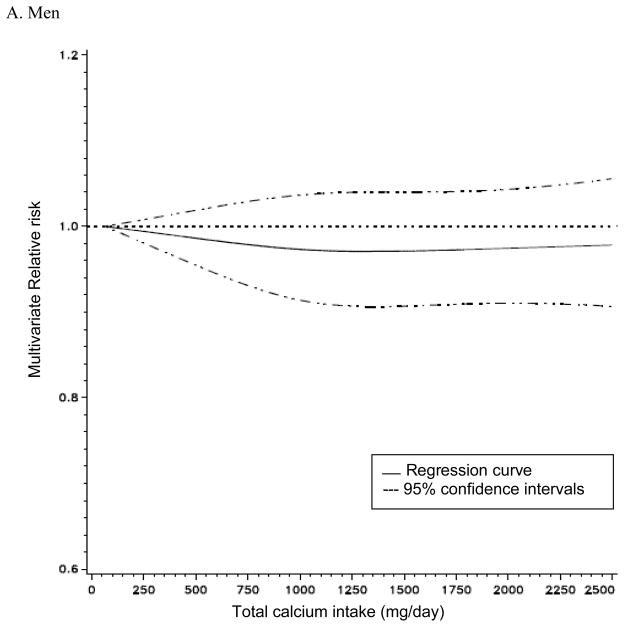
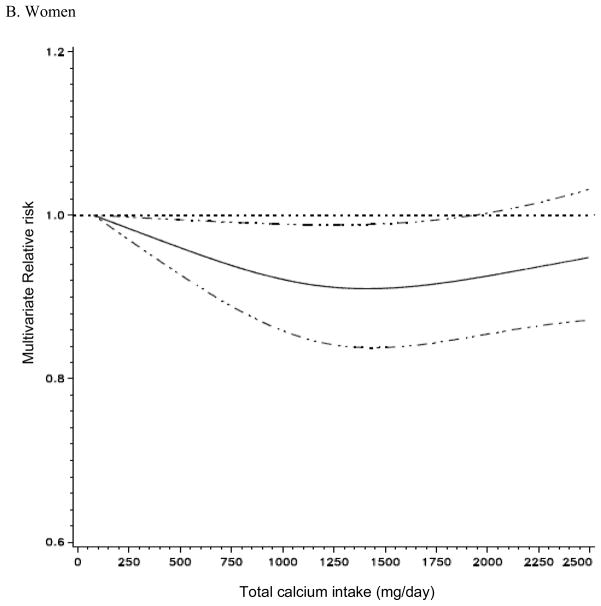
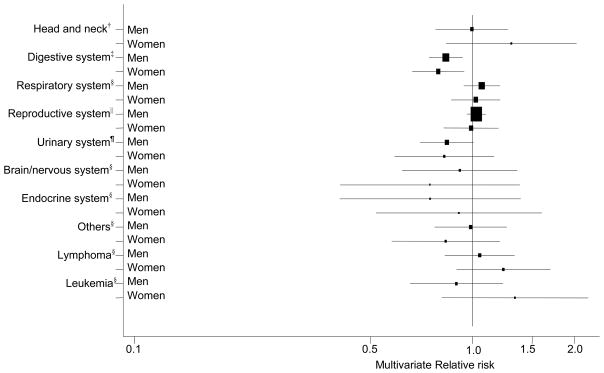
Results: During an average of 7 years of follow-up, we identified 36 965 and 16 605 cancer cases in men and women, respectively. Calcium intake was not related to total cancer in men but was nonlinearly associated with total cancer in women: the risk decreased up to approximately 1300 mg/d, above which no further risk reduction was observed. In both men and women, dairy food and calcium intakes were inversely associated with cancers of the digestive system (multivariate relative risk for the highest quintile of total calcium vs the lowest, 0.84; 95% CI, 0.77-0.92 in men, and 0.77; 95% CI, 0.69-0.91 in women). Decreased risk was particularly pronounced with colorectal cancer. Supplemental calcium intake was also inversely associated with colorectal cancer risk.
Conclusion: Our study suggests that calcium intake is associated with a lower risk of total cancer and cancers of the digestive system, especially colorectal cancer.
Figures
References
-
- Food and nutrition Board. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington DC: National Academy Press; 1997. Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Institute of Medicine.
-
- U. S. Department of Health and Human Services and Department of Agriculture. Dietary guidelines for Americans. 2005. http://www.health.gov/dietaryguidelines/dga2005/document/
-
- Cho E, Smith-Warner SA, Spiegelman D, et al. Dairy foods, calcium, and colorectal cancer: a pooled analysis of 10 cohort studies. J Natl Cancer Inst. 2004;96:1015–22. - PubMed
-
- Moorman PG, Terry PD. Consumption of dairy products and the risk of breast cancer: a review of the literature. Am J Clin Nutr. 2004;80:5–14. - PubMed
-
- Breslow RA, Graubard BI, Sinha R, Subar AF. Diet and lung cancer mortality: a 1987 National Health Interview Survey cohort study. Cancer Causes and Control. 2000;11:419–431. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
