

The new AASM criteria for scoring hypopneas: impact on the apnea hypopnea index
- PMID: 19238801
- PMCID: PMC2635578
- DOI: 10.1093/sleep/32.2.150
The new AASM criteria for scoring hypopneas: impact on the apnea hypopnea index
Abstract
Study objectives: To compare apnea-hypopnea indices (AHIs) derived using 3 standard hypopnea definitions published by the American Academy of Sleep Medicine (AASM); and to examine the impact of hypopnea definition differences on the measured prevalence of obstructive sleep apnea (OSA).
Design: Retrospective review of previously scored in-laboratory polysomnography (PSG).
Setting: Two tertiary-hospital clinical sleep laboratories.
Patients or participants: 328 consecutive patients investigated for OSA during a 3-month period.
Interventions: N/A.
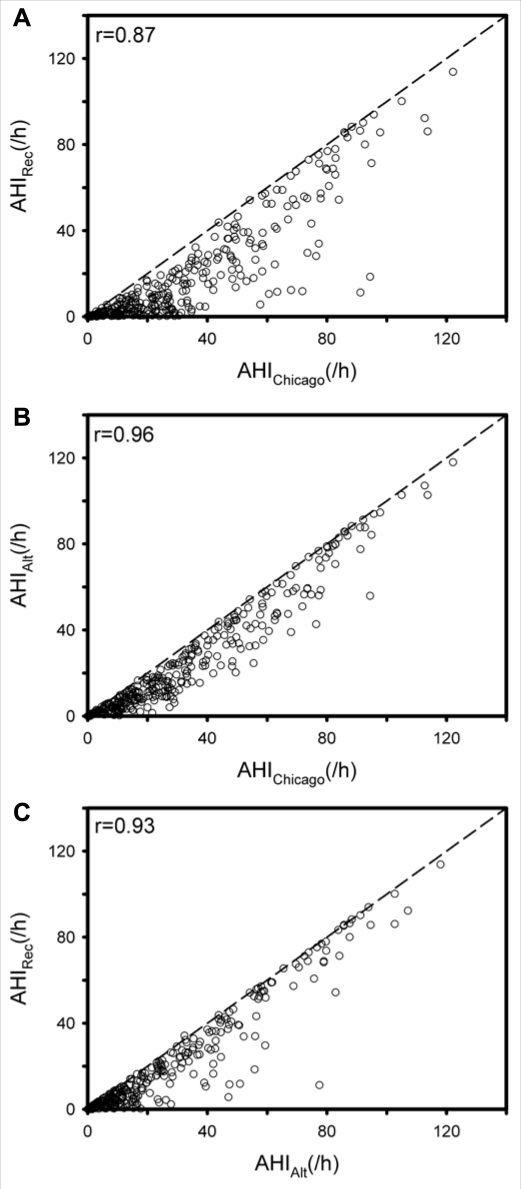
Measurements and results: AHIs were originally calculated using previous AASM hypopnea scoring criteria (AHI(Chicago)), requiring either >50% airflow reduction or a lesser airflow reduction with associated >3% oxygen desaturation or arousal. AHIs using the "recommended" (AHI(Rec)) and the "alternative" (AHI(Alt)) hypopnea definitions of the AASM Manual for Scoring of Sleep and Associated Events were then derived in separate passes of the previously scored data. In this process, hypopneas that did not satisfy the stricter hypopnea definition criteria were removed. For AHI(Rec), hypopneas were required to have > or =30% airflow reduction and > or =4% desaturation; and for AHI(Alt), hypopneas were required to have > or =50% airflow reduction and > or =3% desaturation or arousal. The median AHI(Rec) was approximately 30% of the median AHI(Chicago), whereas the median AHI(Alt), was approximately 60% of the AHI(Chicago), with large, AHI-dependent, patient-specific differences observed. Equivalent cut-points for AHI(Rec) and AHI(Alt), compared to AHI(Chicago) cut-points of 5, 15, and 30/h were established with receiver operator curves (ROC). These cut-points were also approximately 30% of AHI(Chicago) using AHI(Rec) and 60% of AHI(Chicago) using AHI(Alt). Failure to adjust cut-points for the new criteria would result in approximately 40% of patients previously classifled as positive for OSA using AHI(Chicago) being negative using AHI(Rec) and 25% being negative using AHI(Alt).
Conclusions: This study demonstrates that using different published standard hypopnea definitions leads to marked differences in AHI. These results provide insight to clinicians and researchers in interpreting results obtained using different published standard hypopnea definitions, and they suggest that consideration should be given to revising the current scoring recommendations to include a single standardized hypopnea definition.
Figures

References
-
- Manser RL, Rochford P, Naughton MT, et al. Measurement variability in sleep disorders medicine: the Victorian experience. Intern Med J. 2002;32(8):386–93. - PubMed
-
- Moser NJ, Phillips BA, Berry DT, Harbison L. What is hypopnea, anyway? Chest. 1994;105(2):426–8. - PubMed
-
- Manser RL, Rochford P, Pierce RJ, Byrnes GB, Campbell DA. Impact of different criteria for defining hypopneas in the apnea-hypopnea index. Chest. 2001;120(3):909–14. - PubMed
-
- Nigro CA, Rhodius EE. Effect of the definition of hypopnea on apnea/hypopnea index. Medicina (B Aires) 2003;63(2):119–24. - PubMed
-
- Redline S, Kapur VK, Sanders MH, et al. Effects of varying approaches for identifying respiratory disturbances on sleep apnea assessment. Am J Respir Crit Care Med. 2000;161(2):369–74. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
