

Obstructive sleep apnea leads to transient uncoupling of coronary blood flow and myocardial work in humans
- PMID: 19238814
- PMCID: PMC2635591
- DOI: 10.1093/sleep/32.2.263
Obstructive sleep apnea leads to transient uncoupling of coronary blood flow and myocardial work in humans
Abstract
Study objectives: Obstructive Sleep Apnea (OSA) is associated with a poor prognosis in patients with coronary artery disease. We hypothesized that abnormalities of coronary blood flow (CBF) associated with obstructive apneas may predispose patients to ischemia. We aimed to determine CBF during respiratory events in patients with OSA.
Setting: University Hospital.
Patients: Ten subjects undergoing elective percutaneous coronary intervention
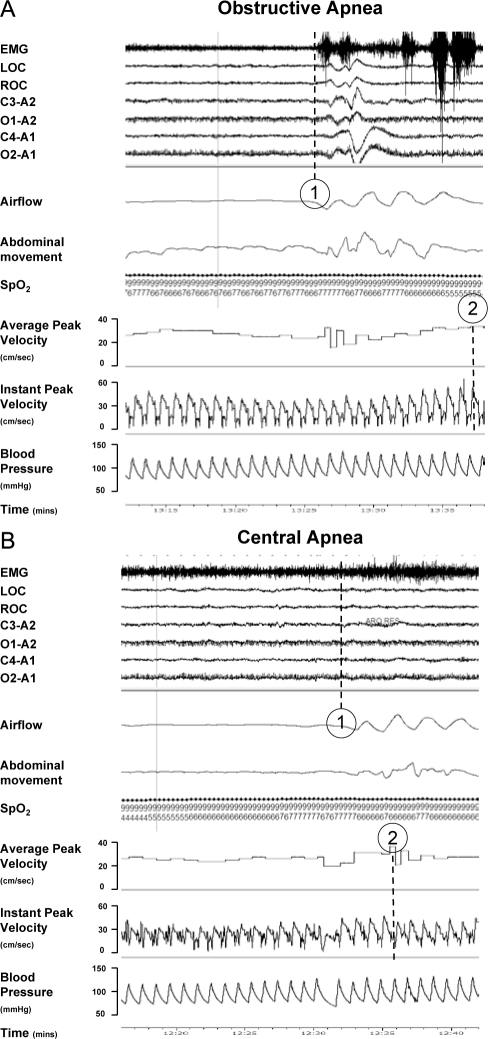
Design: We measured CBF and myocardial work (rate-pressure product [RPP]) in a non-culprit coronary artery in patients sleeping in the cardiac catheterization laboratory. Hemodynamic responses were matched to spontaneously occurring respiratory events.
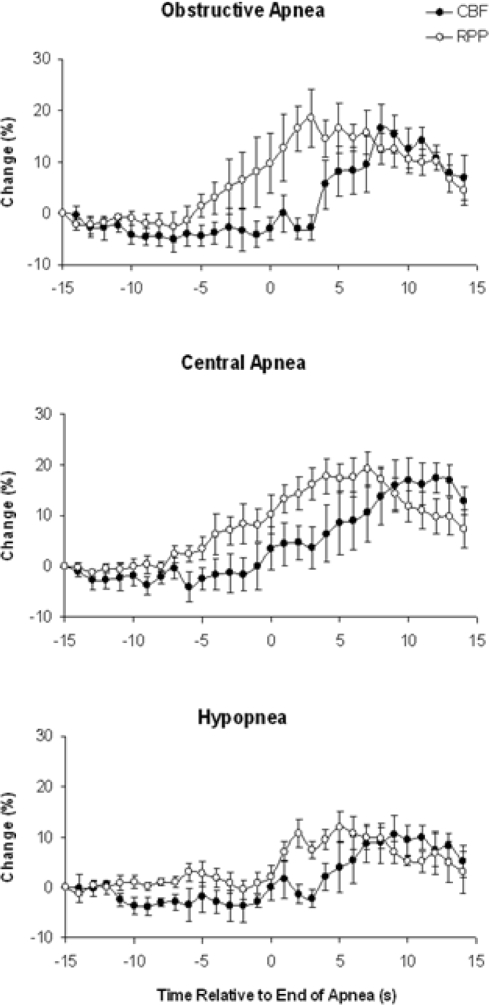
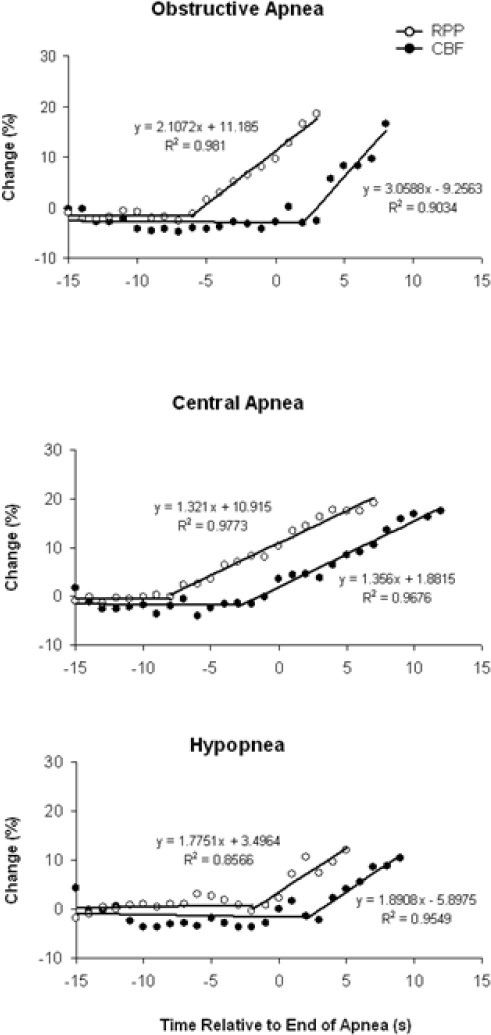
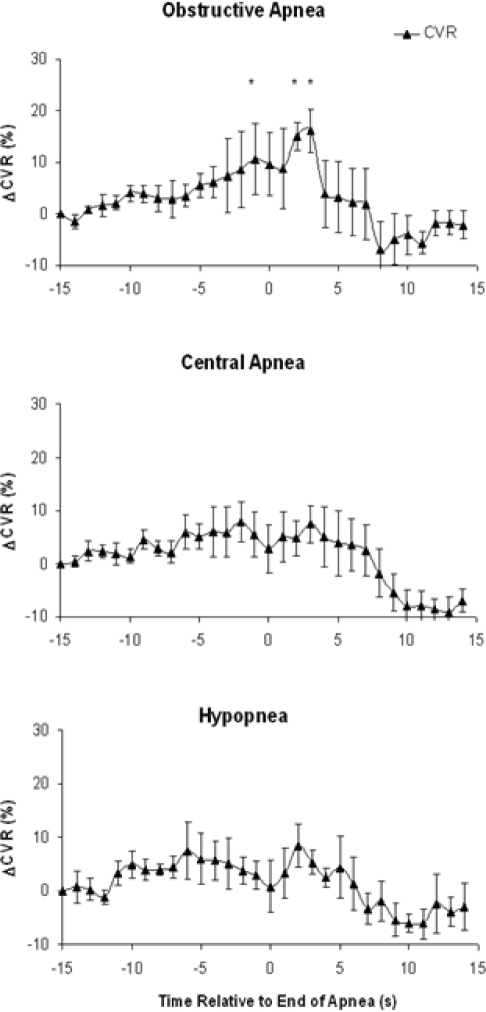
Measurements and results: Events comprised a mixture of obstructive apneas, central apneas and hypopneas. RPP increased at the termination of each type of respiratory event. Following the rise in RPP, there was a delay, identified with breakpoint analysis, before CBF began to increase (P<0.001) that differed in duration with event type: 8 sec for obstructive apnea, 5 sec for central apnea, and 4 sec for hypopnea. The delay in CBF with obstructive apnea was associated with an increase in coronary vascular resistance of 16% +/- 4% (P < 0.05). Stepwise multilinear regression analysis showed the increase in CBF was predicted by the rise in RPP (R=0.52, P<0.001) and presence of arousal from sleep (R=0.30, P<0.05), but not the degree of O2 desaturation.
Conclusion: Following obstructive apneas there is a transient uncoupling of CBF from myocardial work and an increase in CVR. This disturbed flow-metabolic coupling may lead to nocturnal myocardial ischemia in patients with both OSA and coronary artery disease.
Figures
References
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. - PubMed
-
- Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163:19–25. - PubMed
-
- Peker Y, Hedner J, Kraiczi H, Loth S. Respiratory disturbance index: an independent predictor of mortality in coronary artery disease. Am J Respir Crit Care Med. 2000;162:81–6. - PubMed
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. - PubMed
-
- Gami AS, Howard DE, Olson EJ, Somers VK. Day-night pattern of sudden death in obstructive sleep apnea. N Engl J Med. 2005;352:1206–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
