

Intersecting birth weight-specific mortality curves: solving the riddle
- PMID: 19240224
- PMCID: PMC2727223
- DOI: 10.1093/aje/kwp024
Intersecting birth weight-specific mortality curves: solving the riddle
Abstract
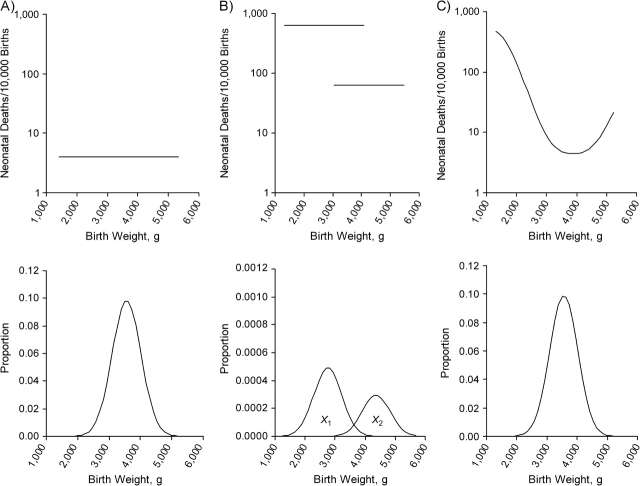
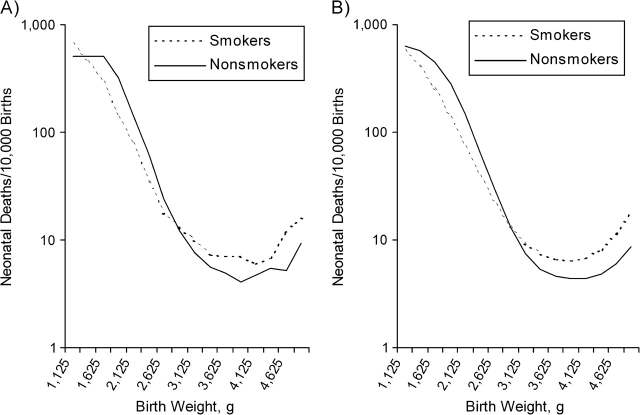
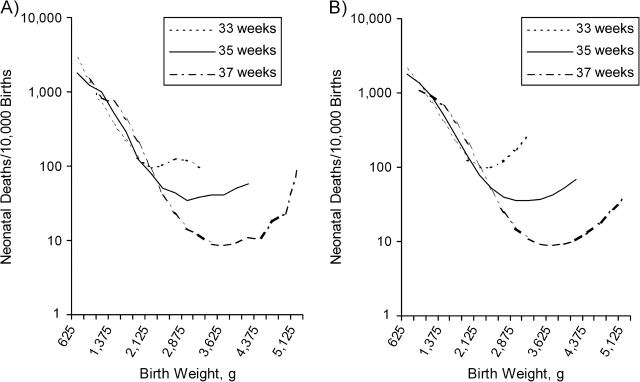
Small babies from a population with higher infant mortality often have better survival than small babies from a lower-risk population. This phenomenon can in principle be explained entirely by the presence of unmeasured confounding factors that increase mortality and decrease birth weight. Using a previously developed model for birth weight-specific mortality, the authors demonstrate specifically how strong unmeasured confounders can cause mortality curves stratified by known risk factors to intersect. In this model, the addition of a simple exposure (one that reduces birth weight and independently increases mortality) will produce the familiar reversal of risk among small babies. Furthermore, the model explicitly shows how the mix of high- and low-risk babies within a given stratum of birth weight produces lower mortality for high-risk babies at low birth weights. If unmeasured confounders are, in fact, responsible for the intersection of weight-specific mortality curves, then they must also (by virtue of being confounders) contribute to the strength of the observed gradient of mortality by birth weight. It follows that the true gradient of mortality with birth weight would be weaker than what is observed, if indeed there is any true gradient at all.
Figures


Comment in
-
Invited commentary: Crossing curves--it's time to focus on gestational age-specific mortality.Am J Epidemiol. 2009 Apr 1;169(7):798-801. doi: 10.1093/aje/kwp025. Epub 2009 Feb 24. Am J Epidemiol. 2009. PMID: 19240223 Free PMC article.
References
-
- Basso O, Wilcox AJ, Weinberg CR. Birth weight and mortality: causality or confounding? Am J Epidemiol. 2006;164(4):303–311. - PubMed
-
- Wilcox AJ. Birth weight and perinatal mortality: the effect of maternal smoking. Am J Epidemiol. 1993;137(10):1098–1104. - PubMed
-
- Hernandez-Diaz S, Schisterman EF, Hernan MA. The birth weight “paradox” uncovered? Am J Epidemiol. 2006;164(11):1115–1120. - PubMed
-
- Haig D. Meditations on birth weight: is it better to reduce the variance or increase the mean? Epidemiology. 2003;14(4):490–492. - PubMed
-
- Wilcox AJ. On the importance—and the unimportance—of birthweight. Int J Epidemiol. 2001;30(6):1233–1241. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
