

Differences between sagittal femoral mechanical and distal reference axes should be considered in navigated TKA
- PMID: 19242764
- PMCID: PMC2866923
- DOI: 10.1007/s11999-009-0762-5
Differences between sagittal femoral mechanical and distal reference axes should be considered in navigated TKA
Abstract
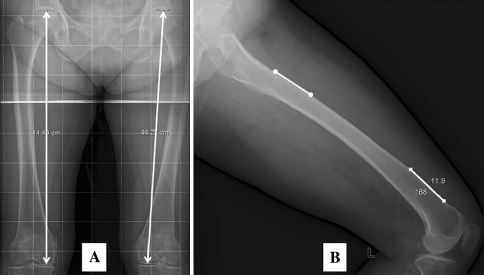
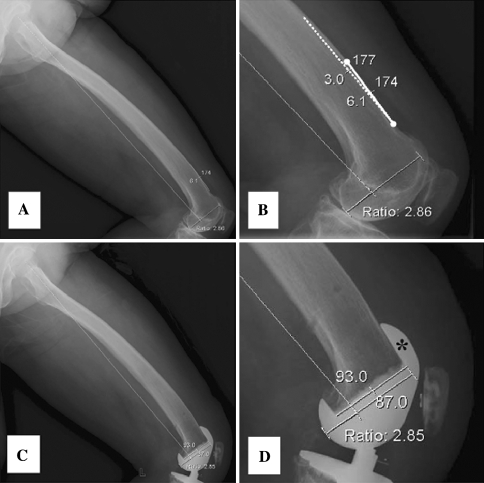
In computer-assisted TKA, surgeons determine positioning of the femoral component in the sagittal plane based on the sagittal mechanical axis identified by the navigation system. We hypothesized mechanical and distal femoral axes may differ on lateral views and these variations are influenced by anteroposterior bowing and length of the femur. We measured angles between the mechanical axis and distal femoral axis on 200 true lateral radiographs of the whole femur from 100 adults. We used multivariate linear regression to identify predictors of differences between the axes. Depending on the method used to define the two axes, the mean angular difference between the axes was as much as 3.8 degrees and as little as 0.0 degrees, with standard differences ranging from 1.7 degrees to 1.9 degrees. Variation between the two axes increased with increased femoral bowing and increased femoral length. Surgeons should consider differences between the mechanical axes and distal femoral axes when they set the sagittal plane position of a femoral component in navigated cases. Our findings also may be relevant when measuring rotation of the femoral component in the sagittal plane from postoperative radiographs or when interpreting femoral component sagittal rotation results reported in other studies.
Figures

References
-
- Brattstrom H. Patella alta in non-dislocating knee joints. Acta Orthop Scand. 1970;41:578–588. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
