

Time-trend of melanoma screening practice by primary care physicians: a meta-regression analysis
- PMID: 19242870
- PMCID: PMC2852745
- DOI: 10.1080/03009730802579620
Time-trend of melanoma screening practice by primary care physicians: a meta-regression analysis
Abstract
Objective: To assess whether the proportion of primary care physicians implementing full body skin examination (FBSE) to screen for melanoma changed over time.
Methods: Meta-regression analyses of available data.
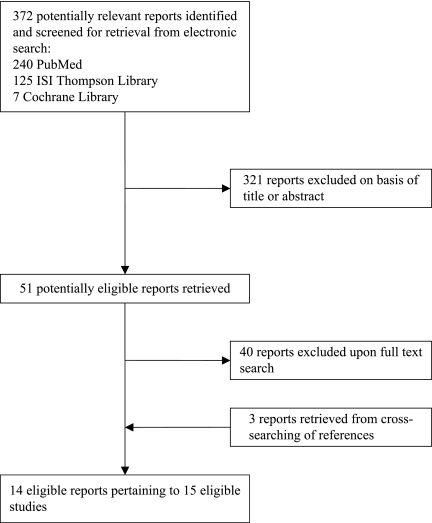
Data sources: MEDLINE, ISI, Cochrane Central Register of Controlled Trials.
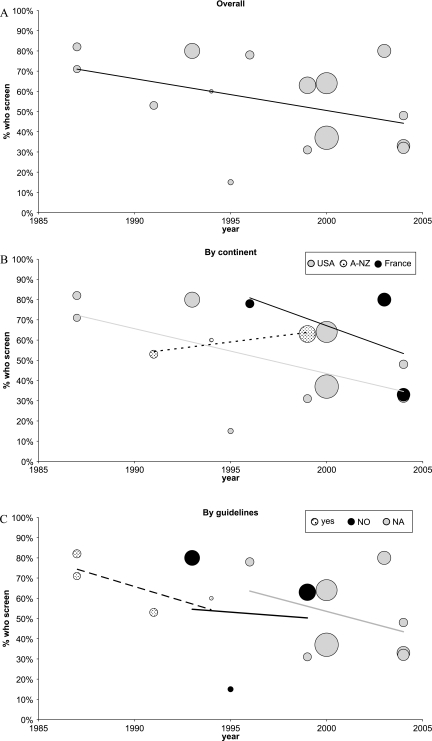
Results: Fifteen studies surveying 10,336 physicians were included in the analyses. Overall, 15%-82% of them reported to perform FBSE to screen for melanoma. The proportion of physicians using FBSE screening tended to decrease by 1.72% per year (P =0.086). Corresponding annual changes in European, North American, and Australian settings were -0.68% (P =0.494), -2.02% (P =0.044), and +2.59% (P =0.010), respectively. Changes were not influenced by national guide-lines.
Conclusions: Considering the increasing incidence of melanoma and other skin malignancies, as well as their relative potential consequences, the FBSE implementation time-trend we retrieved should be considered a worrisome phenomenon.
Figures
Similar articles
-
A Large Skin Cancer Screening Quality Initiative: Description and First-Year Outcomes.JAMA Oncol. 2017 Aug 1;3(8):1112-1115. doi: 10.1001/jamaoncol.2016.6779. JAMA Oncol. 2017. PMID: 28241191 Free PMC article.
-
Overcoming obstacles to skin cancer examinations and prevention counseling for high-risk patients: results of a national survey of primary care physicians.J Am Board Fam Pract. 2004 Nov-Dec;17(6):416-23. doi: 10.3122/jabfm.17.6.416. J Am Board Fam Pract. 2004. PMID: 15575033
-
Melanoma screening: A plan for improving early detection.Ann Med. 2016;48(3):142-8. doi: 10.3109/07853890.2016.1145795. Epub 2016 Feb 25. Ann Med. 2016. PMID: 26911192 Review.
-
Geographic disparities in diagnostic screening for metastatic uveal melanoma.Ophthalmology. 2004 Dec;111(12):2254-8. doi: 10.1016/j.ophtha.2004.06.022. Ophthalmology. 2004. PMID: 15582082
-
Designing tailored Web-based instruction to improve practicing physicians' chlamydial screening rates.Acad Med. 2002 Sep;77(9):929. doi: 10.1097/00001888-200209000-00032. Acad Med. 2002. PMID: 12228099 Review.
References
-
- Ries LAG, Eisner MP, Kosary CL, Hankey BF, Miller BA, Clegg L, et al. Bethesda: MD: National Cancer Institute; 2005. SEER Cancer Statistics Review, 1975–2002. Available from. (accessed March 2008)
-
- American Cancer Society http://www.cancer.org/downloads/STT/2008CAFFfinalsecured.pdf. Cancer facts and figures 2008. Available from: (accessed March 2008)
-
- Young SE, Giulano AE, Morton DL. Three decades of evolving treatment for melanoma: No improvement in survival? J Clin Oncol. 2005;23:7511.
-
- Geller AC, Swetter SM, Brooks K, Demierre MF, Yaroch AL. Screening, early detection and trends for melanoma: current status (2000–2006) and future directions. J Am Acad Dermatol. 2007;57:555–72. - PubMed
-
- Rigel DS, Carucci JA. Malignant melanoma prevention, early detection and treatment in the 21st century. CA Cancer J Clin. 2000;50:215–37. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical